

Introduction
Breastfeeding has significant public health benefits for mothers and infants1, including providing nutrition for neonatal brain development and immunity, emotional and psychological connection between mother and infant, and stress reduction2. These benefits are broadly understood by the Australian community, leading to some of the highest breastfeeding initiation rates in the world1,3. According to the latest data, 90.6% of Australian children aged 0–3 years had received breastmilk; however, only 37.5% were exclusively breastfed to 6 months, which is a key indicator in the national strategy4.
The national breastfeeding strategy confirms the importance of breastfeeding for intergenerational human health and has set national targets for breastfeeding. However, the absence of mandatory, standardised data collection on the rate and duration of breastfeeding conceals the progress, or lack thereof, against national targets1. The determinants of successful breastfeeding to the recommended 2 years and beyond are multifaceted5 and include different levels in the socioecological system6,7: structural policy (culture and other policies), organisational (maternity leave, workplace, hospital), interpersonal and community (partners support, peer and support counselling), and individual factors (knowledge, education, beliefs)8. While the establishment of breastfeeding is thought to occur between 6 and 8 weeks9, the initial crucial period for breastfeeding support is the first 2 weeks10. Midwives are best placed to provide this initial support10 but there are limitations in rural and remote settings, including extensive distances between home and services and resourcing for postnatal care beyond the first 5 days due to challenges in sustaining local community services11, which has made it essential to increase access for women requiring ongoing breastfeeding support12. Women cite reasons such as poor milk supply, their baby’s loss of interest in feeding from the breast and poor breastfeeding support as reasons for ceasing to breastfeed after discharge from the maternity service13. Women living in rural and remote areas have the added barrier of distance from face-to-face support during the early postpartum period, and must often travel large distances to access lactation support once discharged from the service where they birthed1. Geographical health inequities such as access to services close to home, socioeconomic impacts and service planning gaps are added barriers for women living in remote areas 14.
Telehealth describes healthcare services, health education and health information provided by remote technologies such as audio and video equipment15, and has been a general health service delivery model for decades16. With the event of the COVID-19 pandemic, telehealth rapidly moved from being an ad hoc, innovative intervention to being embedded in routine clinical care17-19. The benefits of telehealth include the possibility of increased contact between a consumer and service provider, access to lactation consultants accredited by the International Board of Lactation Consultant Examiners9 and the expansion of health care into rural areas traditionally hard to access20. The COVID-19 pandemic led to a substantial increase in remotely provided maternity care services, including breastfeeding support, making it important to understand whether remotely provided support is effective21.
A recent integrative review reports that, across the world, clinical telehealth interventions have been implemented to support breastfeeding16. Evidence suggests that providing breastfeeding education and support by telehealth can increase exclusive breastfeeding and extend breastfeeding duration. International evidence shows telehealth is perceived as an acceptable and beneficial modality20 that increases access to information and care during critical periods for mothers and newborns16. Programs evaluated under the umbrella of telehealth have been limited by small sample sizes and a lack of standardisation20, and have been conducted outside of Australia. The type of intervention provided to support breastfeeding varies widely in the global evidence and comprises text messages, phone calls, mobile phone applications and structured support combined with educational materials. The providers of these interventions varies from peer supporters with breastfeeding experience to midwives and lactation consultants21. Although there is research into a variety of telehealth breastfeeding services with diversity of providers, there are no Australian studies exploring stakeholder perspectives of accessing or providing lactation consultant services (LCS) by telehealth to women living in rural Australia.
To address this gap, the aim of this study was to investigate stakeholder perspectives of using telehealth to access or provide perinatal education and/or clinical service delivery through the Western Australian Country Health Service (WACHS) Lactation Consultant Telehealth Service (LCTS). This study also aimed to explore the economic impact of using telehealth to deliver clinical services. Stakeholders included consumers, clinicians providing care and clinicians referring to the WACHS LCTS.
Methods
This two-phase multi-methods exploratory study investigated the perspectives of two stakeholder groups: women accessing the LCTS (consumers) and the clinicians referring to and delivering the service (clinicians). Multi-methods research adopts different approaches to discovering new information and was considered ideal to explore discrete perspectives as well as those contextualised by lived experience22,23. The first phase was an online cross-sectional study, which has recognised utility to ascertain discrete information about the phenomena under study at fixed points in time24. The second phase comprised in-depth interviews with consumers and clinicians, and adopted a descriptive qualitative approach useful for eliciting straightforward descriptions of experiences and perceptions of phenomenon under study, grounded in the lived experience of individuals25. To support rigour and transparency in the qualitative component of this study, the backgrounds and relationships of the research team were considered. The interviewer was independent of the clinical service delivery and was not known to either consumer or clinician participants.
Research setting
Western Australia (WA) is one of the least densely populated regions in the world, and the challenges associated with accessing health care are recognised by people living outside of metropolitan areas4. The WACHS is the largest health service by area in the world26, exceeding 2,500,000 km2, with seven regions: Kimberley, Pilbara, Midwest, Goldfields, Wheatbelt, Southwest and Great Southern. This unique setting offers an opportunity to understand the perspectives of those who access telehealth support for breastfeeding, and those referring to or supporting breastfeeding via telehealth, in some of the most remote places on earth.
Survey tools
Owing to the novel nature of this study, there were no validated tools available to explore perspectives of using telehealth to receive or provide LCS. An expert group consisting of a midwife researcher, midwife leaders, service providers, a lived experience expert (consumer), a biostatistician and a health economist collaborated to develop two survey tools: a consumer or lived experience expert (LEE) survey tool and a clinician or healthcare provider (HCP) survey tool (Supplementary material 1 and 2). The surveys collected demographic data and information about experiences of receiving or referring to lactation consultant care by telehealth. At the completion of the survey, participants had the opportunity to express an interest in undertaking an individual online interview to further describe their experience. Each tool was piloted by three consumers and clinicians, after which minor amendments were made; pilot responses were not included in the final data analysis. The surveys were built and managed on REDCap v14.0.2 (Vanderbilt; https://project-redcap.org) on the WA Health server. Respondents were anonymous.
Recruitment
Anyone who had used the LCTS was invited by text message to complete a survey. Mobile phone numbers were obtained under ethics and governance approval by the service. Three text messages were sent to consumers: initial invitation and two reminders. WACHS HCPs were invited to participate via work email address, with one reminder. There were flyers in waiting rooms and staff rooms to publicise the study, with a QR code leading to the survey link for participation.
Sampling
Purposive sampling was adopted; we invited all consumers who had utilised the WACHS LCTS since 2021 and all WACHS regional remote clinicians referring to or delivering the service27,28. In the interview phase, participants who expressed an interest in being interviewed were provided details to a platform to book an interview on a day and time that suited them. Inviting all participants from the survey phase to an interview ensured a range of distribution across WA, range of parity and reasons for accessing LCS29. As an exploratory study, power calculations for the survey phase were not required or undertaken. Sampling for the interview phase was determined by the final number of participants who agreed to interview. Data sufficiency was suspected at eight interviews with four consumers and four clinicians, but a further clinician interview was available and undertaken, which confirmed saturation30.
Data collection
The survey phase involved completion of the online survey by participants between June and August 2023 (13 weeks). Respondents provided informed consent as a hurdle question before being able to gain entry to the survey matter. For the interview phase, guides for LEE and HCP interviews were developed (Supplementary material 3). All who expressed interest were sent an email inviting them to book an interview. Participants provided written informed consent as well as verbal consent prior to interview commencement. Participants were informed that they could decline or answer any questions or withdraw at any time without consequence; the interviewer monitored for signs of distress and would pause or discontinue an interview if needed, with referral to appropriate support services where appropriate. This was not required during interviews in our study. Interviews lasted an average of 26 minutes, and were recorded and transcribed verbatim.
Data analysis
Descriptive statistics were used to report frequencies, and inferential statistics supported tests of association between relevant variables. The economic effects of the service were estimated by converting categorical survey responses regarding cost into a numerical value and then summarising for the entire respondent cohort. Interview data were analysed using a six-step inductive thematic analysis approach31. Two investigators read the transcripts to be familiar with the data; individually generating codes, as a team searched for and reviewed themes, defined and named themes then produced the final report. The first two qualitative analysis steps (data familiarisation and generating initial codes) were undertaken on survey qualitative responses and interview data separately. There was consensus between the two formats, so these were re-analysed as a homogenous data set. To support thematic development and demonstrate the range of responses across survey participants and interviewees, verbatim quotes are presented. Study participants are indicated by a number and a description: survey participants (SP), interview participants (I) consumers (LEE) and clinicians (HCP).
Ethics approval
Ethics and governance approval was provided by WACHS Health Research Ethics Committee (RGS0000005671).
Results
Consumer survey quantitative results
Table 1 presents demographic information and other key characteristics of the 57 consumer survey respondents. Most respondents were aged 26 years and older (94.7%) and spoke English as their first language (94.7%). Just under half the respondents were living in the Southwest WACHS region (45.6%) and reported having to travel further than 60 km to access face-to-face services (44.4%). For more than two-thirds of the respondents, this was their first-time breastfeeding (68.4%). More than one-third of respondents had attended breastfeeding education classes online previously (36.8%). Accessing other lactation support alongside the WACHS LCTS was common among respondents, 45.6% reporting that they were also accessing face-to-face education with a midwife. One-quarter of respondents reported accessing private LCS (24.6%) and social media group support (24.6%). Of the nine (15.8%) respondents who endorsed ‘other’, four (44.4%) reported they were also accessing breastfeeding support from a child health nurse.
Table 2 shows the reasons why respondents sought breastfeeding support from the LCTS. The most common reasons were latching advice (68.4%), followed by first-time breastfeeding (42.1%) and cracked, sore nipples (36.8%). Of the 12 respondents who endorsed ‘other’, five (41.7%) reported issues with supply (eg oversupply, undersupply) and three (25%) reported functional difficulties (e.g. inverted/flat nipples, blocked ducts). Half of the respondents reported that their local maternity service did not offer face-to-face LCS (n=29/57, 50.9%). Most respondents heard about the WACHS LCTS by referral from their midwife, doctor or healthcare service (93%).
Figure 1 displays respondents’ agreement with LCTS technology-related evaluation outcomes. Across the five statements, agreement was strong, with disagreement responses (‘somewhat disagree’ and ‘strongly disagree’ combined) endorsed by few respondents (≤13%). Few respondents were concerned about their internet data usage to access the LCTS (n=3/55, 5.5%). Most respondents reported that they received the support and information they required from the LCTS (89.5%). Nearly three-quarters of respondents felt that the service enabled them to breastfeed their child for longer (78.9%) and 39.3% of respondents felt that they would not have continued breastfeeding their child if they had not accessed the LCTS (n=22/57; Table 2).
The proportion of respondents reporting that the LCTS provided the support and information that they required and the proportion who reported preferring face-to-face LCS by the reasons respondents reported seeking breastfeeding support is displayed in Figure 2.
Most respondents agreed that they would suggest the LCTS to others (87.7%; Table 2). Of the seven (12.3%) respondents who reported that they would not suggest the program to others, the predominant reason was a concern that videoconferencing does not allow adequate support for latching (n=5, 71.4%). Broadly, there was strong support for the LCS via telehealth and almost 90% of respondents reporting they received the required support and information needed from the LCTS. Although face-to-face LCS was not an option for most (in effect a false choice), more than three-quarters of respondents would have preferred that option (77.2%; Table 2).
Table 1: Respondent sociodemographic and other key characteristics for Western Australian Country Health Service Lactation Consultant Telehealth Service Consumer Evaluation Survey (N=57)
| Characteristic | Variable | n | %† |
|---|---|---|---|
| Age (years) | <25 | 3 | 5.3 |
| 26–34 |
33 |
57.9 | |
| ≥35 |
21 |
36.8 | |
| Aboriginal or Torres Strait Islander (missing n=3) | 1 | 1.9 | |
| English first language | 54 | 94.7 | |
| Western Australia region | Great Southern | 8 | 14.0 |
| Southwest |
26 |
45.6 | |
| Goldfields |
1 |
1.8 | |
| Kimberley |
6 |
10.5 | |
| Pilbara |
6 |
10.5 | |
| Midwest |
3 |
5.3 | |
| Wheatbelt |
7 |
12.3 | |
| Distance to travel to reach face-to-face services (missing n=3) (km) | 1–10 | 8 | 14.8 |
| 11–20 |
8 |
14.8 | |
| 21–40 |
5 |
9.3 | |
| 41–60 |
9 |
16.7 | |
| >60 |
24 |
44.4 | |
| First time breastfeeding | 39 | 68.4 | |
| Attended online breastfeeding education previously | 21 | 36.8 | |
| Accessing other lactation support alongside WACHS LCTS | GP | 10 | 17.5 |
| Face-to-face education with a midwife |
26 |
45.6 | |
| Social media groups |
14 |
24.6 | |
| Private LCS |
14 |
24.6 | |
| Friends/family |
21 |
36.8 | |
| Other |
9 |
15.8 |
† Valid %; n=missing removed from denominator.
LCS, lactation consultant service. WACHS LCTS, Western Australian Country Health Service Lactation Consultant Telehealth Service
Table 2: Respondent referral information and evaluation for Western Australian Country Health Service Lactation Consultant Telehealth Service Consumer Evaluation Survey (N=57)
| Characteristic | Variable | n | %† |
|---|---|---|---|
| Reason for seeking LCS | Cracked, sore nipples | 21 | 36.8 |
| Mastitis |
9 |
15.8 | |
| First-time breastfeeding |
24 |
42.1 | |
| Unsettled baby |
16 |
28.1 | |
| Suspected tongue tie |
9 |
15.8 | |
| Baby not gaining weight |
13 |
22.8 | |
| Latching advice |
39 |
68.4 | |
| Other |
12 |
21.1 | |
| Availability of face-to-face LCS at local health service | Yes | 14 | 24.6 |
| No |
29 |
50.9 | |
| Don’t know |
14 |
24.6 | |
| How respondent heard about WACHS LCTS | Referral from midwife/doctor | 41 | 71.9 |
| Requested referral from healthcare provider |
12 |
21.1 | |
| Word of mouth |
5 |
8.8 | |
| Internet search |
0 |
0.0 | |
| Social media |
2 |
3.5 | |
| Flyer/advertising local health service |
2 |
3.5 | |
| LCTS provided the support and information required | 51 | 89.5 | |
| LCTS assisted breastfeeding for longer | 45 | 78.9 | |
| Without LCTS, would not continue breastfeeding | 22 | 39.3 | |
| Would access the LCTS again if needing lactation advice | 51 | 89.5 | |
| Would have preferred face-to-face LCS | 44 | 77.2 | |
| Would suggest the LCTS to others needing breastfeeding support | 50 | 87.7 |
† Valid %; n=missing removed from denominator.
LCS, lactation consultant service. WACHS LCTS, Western Australian Country Health Service Lactation Consultant Telehealth Service.
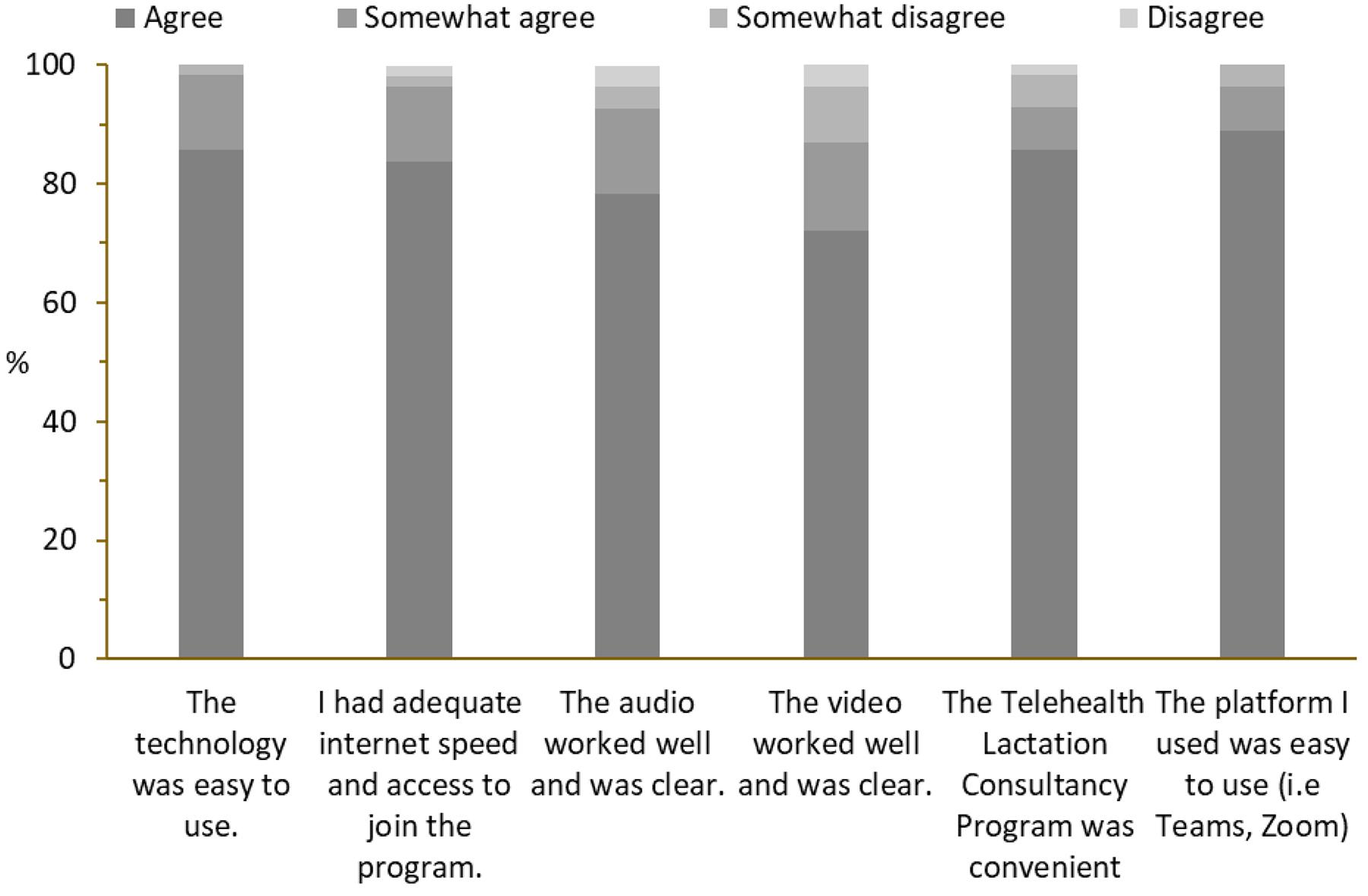 Figure 1: Consumer respondent agreement with Western Australian Country Health Service Lactation Consultant Telehealth Service evaluation statements.
Figure 1: Consumer respondent agreement with Western Australian Country Health Service Lactation Consultant Telehealth Service evaluation statements.
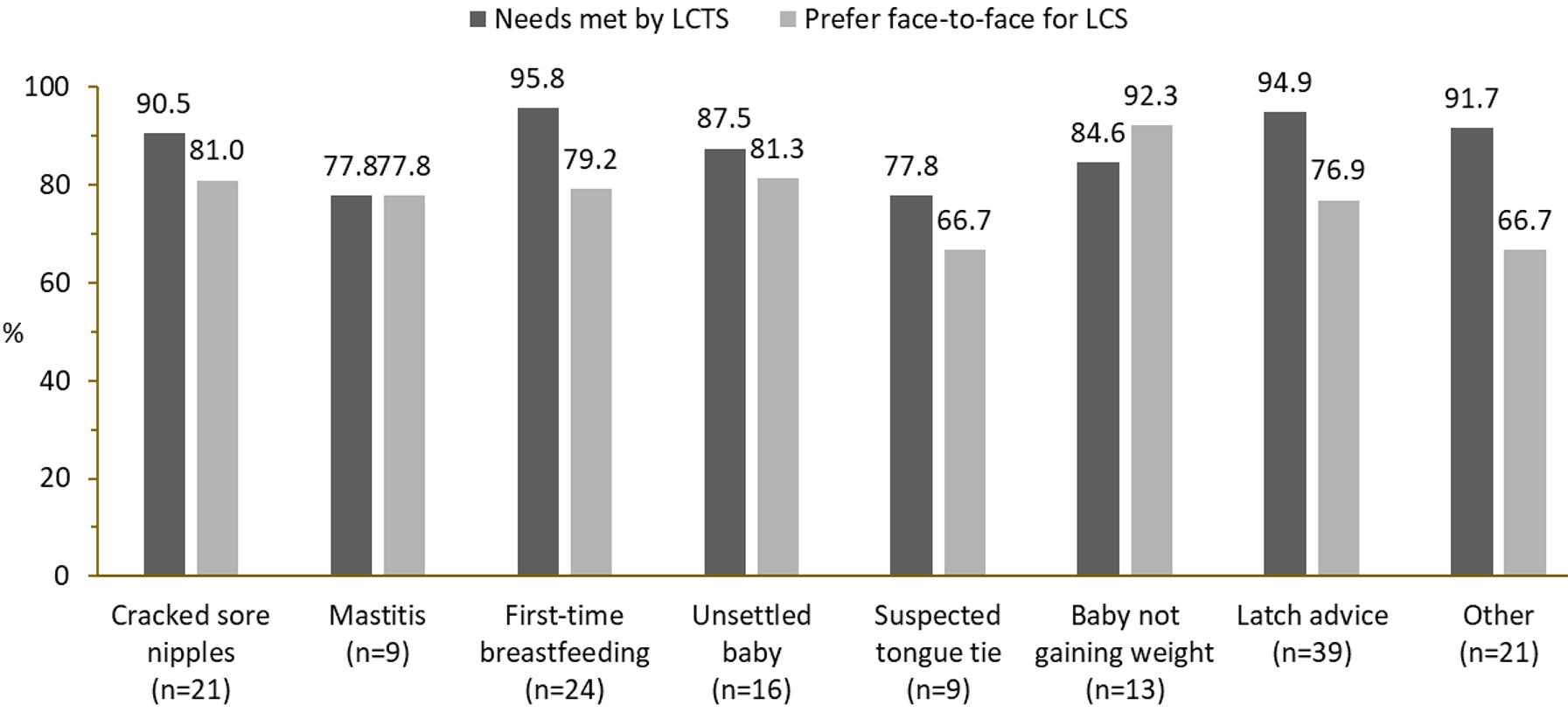 Figure 2: Consumer respondent agreement that their needs for information and support were met by the Western Australian Country Health Service LCTS and that they would prefer face-to-face for LCS, by reported reason for seeking breastfeeding support. LCTS, Lactation Consultant Telehealth Service. LCS, lactation consultant services.
Figure 2: Consumer respondent agreement that their needs for information and support were met by the Western Australian Country Health Service LCTS and that they would prefer face-to-face for LCS, by reported reason for seeking breastfeeding support. LCTS, Lactation Consultant Telehealth Service. LCS, lactation consultant services.
Economic findings
Of the 57 completed economic responses in the consumer survey, 40 (70.2%) stated the service saved them time, with the remaining 17 (29.9%) stating they either did not save time, or they were not sure. Of the 54 responses to the question concerning money, 38 (70.4%) stated they did save money. As an approximation of financial saving, we assumed that each person was at the midpoint of their cost-saving category, with the highest category saving being conservatively A$500; the mean saving per women (including the zero values) is A$168.
The distribution of responses for consumer participants regarding whether they saved time or money is presented in Figure 3.
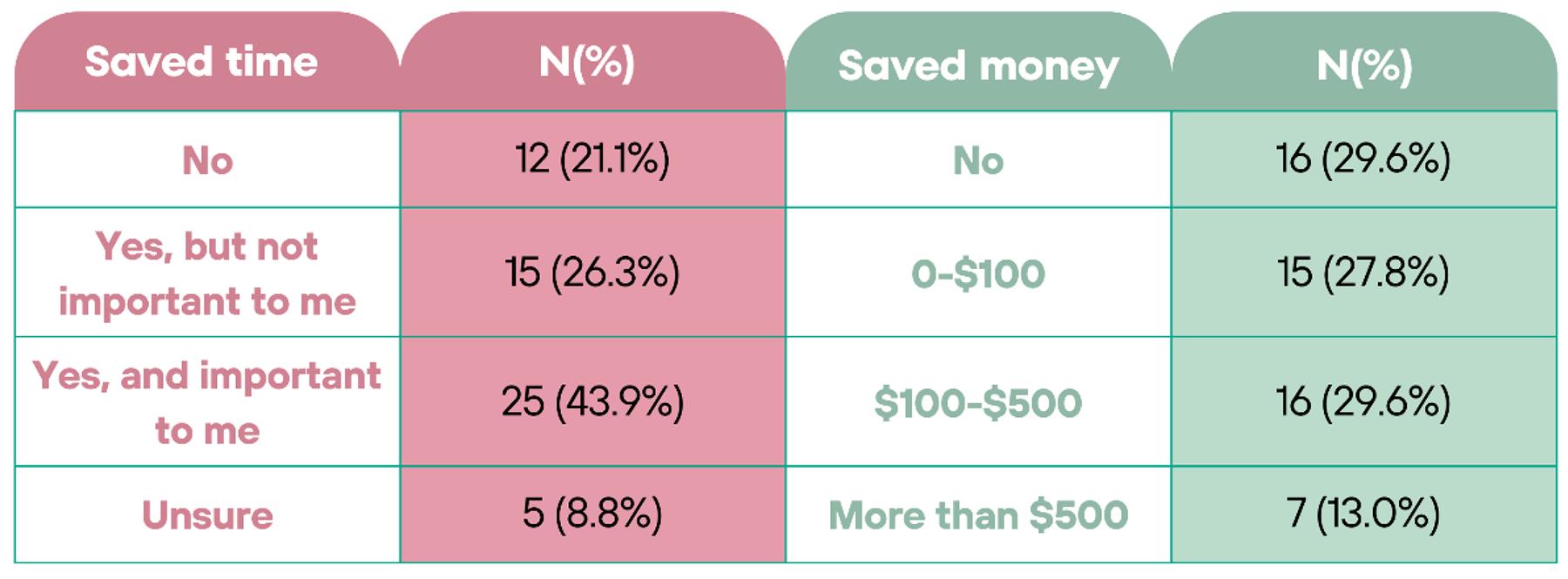 Figure 3: Consumer responses regarding time and money saved using Western Australian Country Health Service Lactation Consultant Telehealth Service.
Figure 3: Consumer responses regarding time and money saved using Western Australian Country Health Service Lactation Consultant Telehealth Service.
Staff survey quantitative results
Table 3 presents demographic information for the 20 clinician survey respondents. Most clinician responses were from midwives (40.0%) and obstetrician/GP obstetrician (25.0%), and more than two-thirds had 11 or more years of experience in their profession (70.0%). The Southwest (40.0%) and Wheatbelt (30.0%) WACHS regions had the largest representation of staff in the survey, and the Goldfields WACHS region had no known staff representation.
Less than half of HCPs indicated that the maternity service at which they were employed offered a face-to-face LCS (42.1%). Clinicians heard about the LCTS most commonly by internal email (85.0%) and word of mouth at their workplace (60.0%). All WACHS clinicians felt that LCTS was a good option for women living in remote regions and almost all respondents felt they were able to help women using telehealth (n=17, 94.5%). Despite this, 13 of 17 respondents thought that LCS delivered face-to-face was more effective for women living in regional centres (76.5%). Further, almost three-quarters of respondents felt that the LCTS is not accessible for all women, including those from non-English speaking backgrounds, those with a disability or those facing social disadvantage (n=13/18, 72.2%). Almost half of the clinicians would have preferred a combination of telehealth and face-to-face delivery methods for the LCS (n=8/17, 47.1%), while almost half again preferred face-to-face LCS only (n=8, 47.1%) and one respondent preferred telehealth LCS only (n=1, 5.9%).
Table 3: Professional and demographic summary of respondents to the Western Australian Country Health Service Lactation Consultant Telehealth Service Staff Evaluation Survey (n=20)
| Characteristic | Variable | n | %† |
|---|---|---|---|
| Profession (missing n=4) | Midwife | 8 | 40.0 |
| Obstetrician/GP obstetrician |
5 |
25.0 | |
| GP |
3 |
15.0 | |
| Other (please specify below) |
4 |
20.0 | |
| Time in profession (missing n=4) (years) | <5 | 3 | 15.0 |
| 6–10 |
3 |
15.0 | |
| 11–15 |
6 |
30.0 | |
| 16–20 |
1 |
5.0 | |
| ≥20 |
7 |
35.0 | |
| Western Australia region (missing n=4) | Great Southern | 2 | 10.0 |
| Southwest |
8 |
40.0 | |
| Goldfields |
0 |
0.0 | |
| Kimberley |
2 |
10.0 | |
| Pilbara |
1 |
5.0 | |
| Midwest |
1 |
5.0 | |
| Wheatbelt |
6 |
30.0 | |
| Aboriginal or Torres Strait Islander (missing n=4) |
0 |
0.0 |
† Valid %; n=missing removed from denominator.
Qualitative findings
The online surveys provided qualitative data from 71 participants: 55 lived experience experts and 16 HCPs. Nine participants were interviewed: four consumers and five referring clinicians.
Two overarching themes were identified in the qualitative data: ‘clinical service delivery’ and ‘service logistics and sustainability’. Themes and corresponding subthemes are shown in Figure 4.
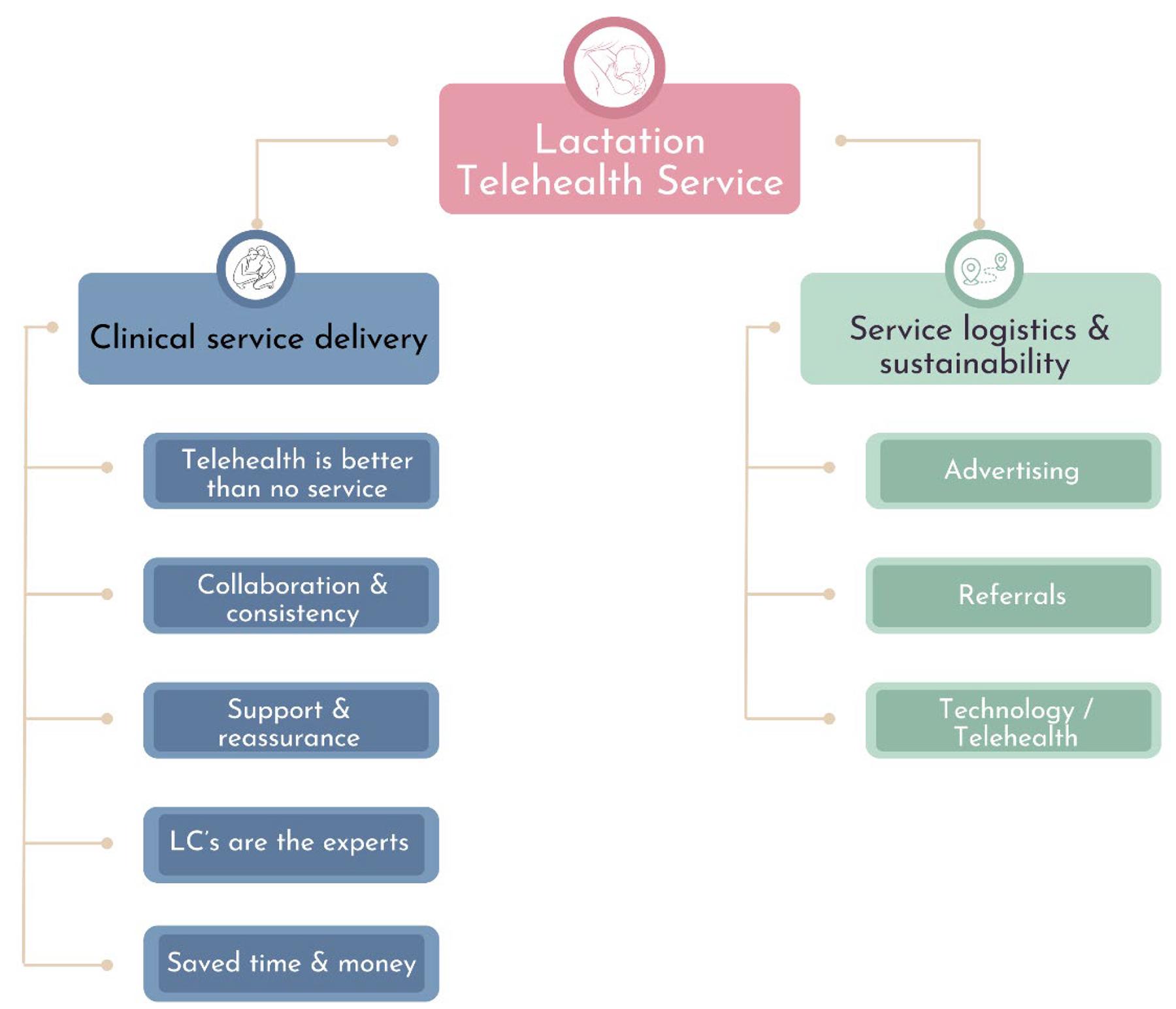 Figure 4: Themes and subthemes for qualitative data from surveys and interviews.
Figure 4: Themes and subthemes for qualitative data from surveys and interviews.
Clinical service delivery
This overarching theme described how the service was delivered to women in regional and remote WA. five subthemes were identified under clinical service delivery:
- telehealth is better than no service
- collaboration and consistency
- support/reassurance
- lactation consultants are the experts
- saved time and money.
Telehealth is better than no service
Many women found the telehealth mode of delivery convenient, and an acceptable alternative to in-person support: ‘After birth, in-person support should be available but if it can’t be then telehealth is the next best thing’ (SP LEE11). There was an agreement that face-to-face was preferred to the telehealth mode of delivery to provide LCS; however, most agreed that the LCTS was better than no service at all for women living in regional/remote WA: ‘My initial sort of response in being offered telehealth was, I was really grateful and appreciative that there was an option, but I would have really preferred to have had something face-to-face’ (I LEE6).
Collaboration and consistency
It was reported that the WACHS LCTS provided consistency in messaging, trust and a plan for women to follow. This was valued by women as they felt that inconsistent advice was given from various HCPs: ‘Switching between the hospital midwife and the child health nurse the first time was confusing and not a pleasant experience. They said different things, and this was not supportive at a time that I needed a lot of support’ (SP LEE11). Another woman said, ‘It really helped me a lot … consistency of information. [The lactation consultants are] knowledgeable, an authority, because you're really – you don’t know, do you? As a first-time mum. It’s really vulnerable [time], and so when people are telling you different things, it just doesn’t help at all’ (I LEE5).
Women also recognised the challenges of delivering consistent messages acknowledging breastfeeding is a deeply personal and individual experience.
There is numerous ways and techniques to breastfeed and as a new mum you’re shown a lot. None are wrong, they’re just different and you should go with the technique that works for you and that’s ok. (SP LEE53)
Support/reassurance
This subtheme described how the WACHS LCTS met the needs of supporting and reassuring women and, in some cases, resulted in women being able to feed for longer.
The service was absolutely amazing, and we may not have managed to get breastfeeding to work without it. Our baby had a tongue tie and refused to latch for over one month after birth. The lactation consultants were so positive, and supported us over those difficult first weeks, meaning that we managed to persevere and now ten months on we’re still breastfeeding. (SP LEE21)
When the WACHS LCTS was provided in conjunction with face-to-face clinical care, clinicians felt the service was able to provide support upskill and provide care to women.
[I] have found the experience so far as excellent, with improved outcomes supporting mothers with breastfeeding issues. Also supportive with up-skilling and enhance midwives’ knowledge when LC [lactation consultant] combines an appointment with the mother and midwife when needed for added support. (SP HCP8)
Clinicians and women discussed a need for improved breastfeeding education, clinical support and reassurance for women living remotely. A consistent theme was to provide the service not only during the first 6 weeks but beyond.
If I recall correctly, this service was available only if accessed in the first 7 weeks after birth, and I believe would be great if that period could be extended. (SP LEE8)
Some felt there were service limitations, suggesting that timely access and the mode of telehealth were barriers.
It was very difficult to assess latch etc via video call and difficult to feed baby and show this on the camera. (SP LEE32)
Lactation consultants are the experts
This subtheme described the benefits of having access to expert advice and the trust that women have in the lactation consultant as an authority on breastfeeding and reported feeling privileged to have this support.
[with my first baby] There was no lactation consultant support in Broome for my first breastfeeding experience and I suffered through 3 months of mastitis. I requested the referral to the lactation consultant the second time around and was very happy with the support provided. I think breastfeeding is underplayed as natural and far more information and support for what to expect should be offered during pregnancy. (SP LEE11).
Saved women time and money
Women described that the LCTS saved them time and money as they were able to access support from home without the need to travel or to seek private support.
… for me to go to the city and have an appointment or even just to a few towns over to have an appointment, that’s taking three extra kids in the car and lunch or potentially overnight accommodation ... It’s potentially hundreds of dollars just for the travel, let alone anything else that comes with it. (I LEE4)
Service logistics and sustainability
Service logistics and sustainability described how the WACHS LCTS is promoted and operated. Subthemes were advertising, referrals and technology.
Advertising
Both clinicians and consumers reported that the advertising of the WACHS LCTS could be improved. It was described that in regional areas there is higher staff turnover and agency staff, which could lead to clinicians being unaware of the service and thus not passing information onto women.
I felt as though she [child health nurse] wasn’t really aware of it until I brought it up with her … if they’re not keeping up [to date] with what’s available, they’re not gonna be able to tell anyone else. (I LEE4)
Referrals
For many consumers, the referral process was simple: a clinician made the referral, then they awaited contact from the LCTLS.
Even when I first reached out and said this is a service I need and I was told you need a referral, it was all with kindness and concern … I didn’t feel like a hassle. I didn’t feel like it was too hard … I was in an appointment so much faster than I anticipated. I was on track and reassured within a couple of days … A lot of the time living out here, accessing health services sometimes feels like it’s too hard. This was not … (I LEE4)
Participants described a need to accept referrals after the baby’s age is 7 weeks.
I think cutting off support at 6 weeks is too early. My bub is 7 months and I have had feeding issues on and off the whole time and nearly given up numerous times. (SP LEE2)
Technology and telehealth
Explorations of the positive and negative aspects of the use of telehealth in providing lactation support for regional and remote women were described in the technology subtheme. Women described convenience, the accessibility and ease of telehealth.
It wasn’t big or daunting. It’s like a phone call, its way more accessible … No, I definitely think telehealth was preferable to anything else, you’ve just had a baby. You don’t wanna be packing stuff up and travelling for God knows how long to get to somewhere and then potentially having to stay and be in an unfamiliar place or where you don’t have the support that you would ordinarily have. You’re not in your comfort zone. (I LEE4)
Another LEE discussed the benefits of face-to-face, but preferred telehealth due to convenience: ‘Might be easier to position baby but overall online was more convenient due to my location’ (SP LEE16). Another woman described the ease of telehealth: ‘I liked online, it was quick and easy. We had enough face-to-face support in the hospital, so we just needed some basics before birth to be prepared’ (SP 54).
Participants discussed challenges juggling babies, phones and other children, all while trying to breastfeed and receive support from the lactation consultant on telehealth: ‘I found it really hard to use video technology while holding my baby/attempting to breastfeed. It was hard for the lactation consultant to see my latch as I couldn’t hold the phone in the right spot one-handed. It became stressful’ (SP LEE35). From the clinician perspective it was also discussed telehealth can make it difficult to perform a clinical assessment: ‘Visualising a feed during a consultation may not always be as optimal as in person’ (SP HCP8).
Access to good-quality internet, technology and video capabilities is vital for an effective service. One local midwife described supporting a woman with a lactation consult via telehealth.
I guess particularly for us up here with access to technology sometimes being quite a barrier or stable internet and different things like that. That’s a big barrier. So, a lot of time we’d co-facilitate that session. (I HCP3)
There were concerns from clinicians that telehealth could be a barrier to receiving lactation consultant support for those women from different cultural and non-English speaking backgrounds.
[telehealth is] extremely difficult for women who speak English as a second language, very difficult for low socioeconomic families who might not have a phone, email account, internet etc – hard for Indigenous families who might prefer face-to-face consults to build rapport and trust. (SP HCP14)
Discussion
This study is the first to explore the perspectives and experiences of key stakeholders of a LCTS in WA, the world’s largest area health service. The geographical spread experienced by participants is a unique component of this study and provides insights into the utility and acceptability of such a service.
Findings from our study indicated that, to be able to address common breastfeeding challenges, women reported that their needs were met by telehealth. These findings are consistent with a systematic review and meta-analysis of remotely provided breastfeeding support studies around the world indicating remote support is an effective intervention for breastfeeding continuation21. Our study identified a preference for in-person lactation consultant support; however, research shows that in regional and remote Australia this isn’t always an option due to limitations in delivering sustainable face-to-face health care32. Our study provides evidence to support the need for both modes of delivery to meet the needs of women living rurally and remotely, noting that where there may not be capacity to do so, a telehealth service can meet the needs of most women.
The period of breastfeeding establishment is recognised as an especially important time in early parenthood that requires support. Midwives are equipped to provide routine breastfeeding support and troubleshooting; however, some persistent or complex challenges of breastfeeding require assessment and support by a lactation consultant9. The WACHS LCTS is staffed by two lactation consultants, enabling consistent education and advice and experienced as supportive by the breastfeeding women in our study. Consistency of support coupled with convenient and timely access through telehealth lactation support is known to improve breastfeeding continuation33. Qualitative data confirmed that maternal confidence was built by consistent advice and messaging.
Continuity of midwifery care is associated with higher breastfeeding rates34 – in WACHS, women are generally transferred from midwifery care to child health, between birth and 10 days of infant age unless they are receiving midwifery continuity of carer through a midwifery group practice model where care extends up to 6 weeks. During this transfer of care, the universal child health schedule service after 14 days is at 2, 4 and 12 months, which limits local access to clinical breast-feeding support. Physical distance can also impact access to clinical care35. Findings of our study have confirmed this gap in service provision, with many participants stating they want more support, and beyond 6 weeks21. Our study shows that a LCTS is an acceptable and feasible option to close this gap for rural mothers. Further implementation research is needed to explore the benefits of a LCTS beyond 6 weeks to the period of 6 months, which is the target for exclusive breastfeeding in the national strategy.
The participant responses suggested that a significant proportion of women saved either time or money or both through provision of the service. This is important as both can be significant barriers in seeking and receiving appropriate lactation support. While our sample was not large enough to determine which women were more likely to face such obstacles, it is likely that these individuals may also be more likely to have characteristics such as lower socioeconomic status and remoteness, common predictors of low initiation and maintenance of successful breastfeeding. Previous research into system cost savings found that early weaning could cost $60 million to $120 million to Australian hospitals annually36 due to hospitalisation costs relating to gastrointestinal illness, respiratory illness, otitis media, eczema and necrotising enterocolitis36,37. Our data shows that the LCTS prevented 39.4% of women from early cessation of breastfeeding, with corresponding expected savings to the health system. The inclusion of an economic analysis highlights the critical role of equitable, sustainable telehealth service provision in improving access to care for women living in rural and regional areas, where geographical distance, cost and service availability continue to shape health outcomes38.
This study has highlighted the preferences of many women and clinicians for face-to-face clinical lactation support, which enables clinicians to physically assess mother and baby (eg for hydration and weight), and observe interactions. Despite the strong preference for face-to-face care, it was established that the telehealth mode of delivery was an acceptable alternative for majority of participants. Findings from our research indicate barriers to telehealth clinical service delivery can be mitigated with clear communication, and collaboration with other care providers and ensuring access to technology. Breastfeeding is a unique example where the woman is holding her baby, her breast a telehealth video device to allow a clinician to observe attachment/latch, the key area of breastfeeding support requested. Strategic investment in telehealth should be accompanied by parallel exploration of improving accessibility of quality care via telehealth for those with disability to ensure access to timely, quality assessment and care39.
There is acknowledgement that the expansion of telehealth services should be inclusive and accommodate those with recognised disadvantage40. Our study has shown stakeholder concern for telehealth accessibility for women who speak languages other than English41,42, those without access to stable technology and with low levels of digital literacy43. Further research is warranted into the effectiveness and clinical outcomes associated with using telehealth to provide health care, including clinical breastfeeding support. Low socioeconomic groups and those living remotely can face difficulty accessing telehealth services – simply accessing a phone or computer technology can be a barrier. Further research is needed to identify which access reasons and clinical concerns are suited to telehealth versus in-person care, to inform evidence-based service design and triage pathways. The development and evaluation of hybrid or flexible models of care to mitigate accessibility barriers and ensure telehealth services are equitable and responsive to diverse consumer needs is vital. Culturally appropriate breastfeeding support is also critical for Aboriginal women and children in WA, and telehealth services should be tailored to respect cultural practices, promote engagement and support equity in maternal and child health outcomes44.
An identified solution from our study is to ensure there is someone available on the ground to cofacilitate sessions where they can assist women, provide stable technology (good internet speed and camera/devices) and to provide the clinical hands-on support many women require. While a validated telehealth evaluation tool was not utilised in this study, our approach was designed to address the specific objectives of this study. Future research may consider incorporating established instruments to enhance standardisation and comparability of findings across different settings.
Strengths and limitations
Our study explored the perspectives of stakeholders from one of the largest health services in the world (by area), providing a unique perspective on the challenges of delivering and accessing care in rural and remote area.
Clinicians outside of WACHS – such as private midwives, private GPs, private lactation consultants and speech therapists – were not personally invited to participate in this study. Only those with a government staff email were invited to participate. The data were collected from women who participated in the service from its inception and therefore some of the earlier feedback around service design and access may not have been reflective of consumer experiences now. Nonetheless, we present the data without alteration to ensure rigour of the study despite it potentially not being a full reflection of the service today.
Despite all women who had accessed the service being invited to participate, the perspectives around culturally and linguistically diverse and Aboriginal women using the service were mainly reported by clinicians rather than from the women themselves. Further research specifically engaging these populations to ascertain the utility of LCTS is warranted.
Conclusion
Despite national recommendations, a strategy and targets to exclusively breastfeed for baby’s first 6 months of life, women can experience challenges if there is no ongoing quality education and clinical support. In addition, rural isolation, distance and unsustainability of face-to-face services can lead to challenges in establishing and maintaining breastfeeding. Our study findings confirm that, despite the desire for face-to-face services, education and clinical service delivery by telehealth is a viable and successful alternative to women travelling to where face-to-face LCS are offered. In some cases, telehealth was preferred over face-to-face care due to convenience and saving the woman money. Where possible, LCS should be offered face-to-face, and the WACHS LCTS can provide an alternative mode of assessment, support and clinical guidance for those living in remote areas. Recommendations for further research and for improving service accessibility have been provided. Findings offer utility for policymakers, service providers and women to support an evidence-informed understanding of the experiences of accessing or referring to lactation consultancy by telehealth.
Acknowledgements
The authors would like to acknowledge and thank the individuals in WACHS who participated in this study.
Funding
No external funding was received in the development and conduct of this research, which was a collaboration between WACHS and Curtin University.
Conflicts of interest
The authors have no conflicts of interest to declare.
AI disclosure statement
We, the authors of this article, declare that no AI or AI-assisted technologies were used in the development of the article.