







Introduction
Type 2 diabetes mellitus is recognized as a public health problem1,2. In middle-to-low-income countries like Brazil, only 37% of people with type 2 diabetes are receiving treatment, and among this group only 23% achieve adequate disease control3,4. In this context, lifestyle modifications emerge as an essential strategy in combating the type 2 diabetes epidemic5,6. These include focusing on regular physical activity, adopting a balanced diet, and adhering to prescribed medications7-10.
Physical inactivity is more prevalent in countries with greater income inequality, regardless of whether they are high or middle income11. Thus, promoting physical activity should avoid exacerbating inequalities such as those relating to geography, age, and gender, and a multisectoral effort has also been recommended12. To achieve the goal, primary health care (PHC) is a strategic setting, as its fundamental premise is to be accessible to all people and offer multisectoral health and wellness services closer to individuals, families, and communities. A fundamental pillar of this level of health is ensuring that care is person-centered, respecting needs and preferences13.
PHC is the strategic level of health systems due to its capacity for accessible services, close to individuals, families and communities, in addition to coordinating intersectoral actions to promote wellbeing14. In Brazil, it is mainly organized through PHC units, where multidisciplinary teams, including community health workers (CHWs), provide longitudinal follow-up and person-centered care, respecting needs and preferences15. Because of their structuring role in the management of chronic conditions, such as type 2 diabetes, PMC units constitute the priority setting for this study.
Adopting healthy physical activity habits remains a significant challenge for individuals with type 2 diabetes. Although this issue is a central focus of management strategies implemented by PHC teams, no substantial improvements have been observed at the population level in vulnerable areas like the Brazilian Amazon16,17. Despite receiving guidance on the importance of physical activity, individuals with type 2 diabetes often show limited behavioral change where low levels of physical activity and failure to meet the recommended guidelines for regular practice have been documented18.
Such non-adherence to physical activity and treatment recommendations compromises disease management, undermines professional–patient relationships, and contributes to increased healthcare costs19. The practice of physical activity is influenced by a complex interaction of factors that can both encourage and hinder adherence20,21. Given this scenario, there is a clear need to explore the contextual factors that influence adherence to physical activity among individuals with type 2 diabetes, particularly in socially vulnerable regions. This study aimed to understand the barriers and facilitators to physical activity adherence in a vulnerable population with type 2 diabetes in the Brazilian Amazon setting.
Methods
Study design
This qualitative approach study, with a participatory interface, is embedded in the matrix project ‘Intervention led by community health agents for the management of type 2 diabetes in the interior of the Amazon’, led by Elisa Brosina de Leon. This research used the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist.
We conducted an exploratory qualitative study using a phenomenological approach. This choice was guided by ontological and epistemological objectives focused on understanding the lived experiences of individuals with type 2 diabetes in relation to adherence to physical activity, and not by a cultural description of lifestyle. This approach seeks to capture the essence of the experience22, suspending preconceived judgements (epoché) and valuing the intersubjectivity between researcher and participant23.
Study setting
The research occurred in a rural city of Amazonas, Iranduba, in the North Region of Brazil, which has a population of approximately 61,000 and is 38 km by car from the regional capital of Manaus. The region is home to many Indigenous communities, which are an integral part of the cultural and historical richness of the Amazon. In recent years, Iranduba has faced extreme climatic events. The combination of heat, smoke, and low rainfall constitutes one of the most challenging periods in decades for the local climate. The city was chosen for the study because its cultural and sociodemographic context are comparable with other cities in Amazonas.
Participants
Data collection was conducted at six PHC units of Iranduba, within a 30 km radius of the Municipal Health Secretariat headquarters. The study population comprised individuals with type 2 diabetes and CHWs engaged in PHC.
For the CHWs, we included only active professionals linked to the six PHC units, excluding those on vacation or leave. For patients with type 2 diabetes, we included adults (aged 18 years or more) diagnosed at least 6 months prior, linked to the same PHC units and followed by the participating CHWs; those whose physical, intellectual, or communicative capacity precluded participation were excluded. In the individual interviews, we applied the same criteria, as well as the requirement of not having previously participated in the World Café (see Data collection below), in order to broaden the diversity of experiences. These criteria ensured methodological coherence and allowed access to different experiences relevant to the phenomenon studied.
Age eligibility was verified through the user registration database available at the PHC units, which identifies those aged 18 years or older. Those unable to travel to the data collection site, which would prevent participation in the World Café, were considered ineligible for the study. Conditions such as arthralgia, although present in many participants, did not constitute an exclusion criterion, as these did not prevent participation in the proposed activity and were part of the barriers experienced in daily care, and therefore relevant to the phenomenon investigated.
The recruitment process was coordinated with the municipal administration. Initially, the team met with the coordination of the municipal health department and subsequently visited the six PHC units to present the project to the coordinators and the CHWs. After this stage, we held an online meeting and created a WhatsApp group to facilitate communication and clarify doubts. The CHWs, knowing their assigned population, compiled a list of patients with type 2 diabetes and invited them directly during home visits or routine contacts. This process ensured an ethical, organized approach aligned with the prior relationship between CHWs and the community.
Data collection
Data collection employed two techniques: the World Café and semi-structured interviews. The process began with the World Café dynamic, titled Prosa e Café. This creative methodology fosters dialog among participants, encouraging collective and collaborative reflections on issues of significant relevance24. On the first day, individuals with type 2 diabetes met in the morning to discuss barriers to physical activity adherence, while CHWs participated in the afternoon. On the second day, using the same approach, discussions focused on facilitators of physical activity adherence. The scheduling of these meetings was organized to align with the operational routines of PHC services.
The first meeting addressed the barriers to adherence to physical activity practice in people with type 2 diabetes and the second focused on facilitators for adherence to physical activity practice in people with type 2 diabetes? Participants also answered a sociodemographic characterization questionnaire. Finally, participants shared their findings in a plenary session. The CHWs were engaged by phone, WhatsApp, and a virtual meeting. They provided a list of 50 participants with type 2 diabetes who met the study’s criteria.
Semi-structured interviews were conducted to gather more in-depth data. Semi-structured interviews were applied exclusively to patients with type 2 diabetes who did not participate in the World Café and who, according to the CHWs, had greater difficulty in adhering to healthy habits. The script used for this group was developed specifically for the individual stage and structured in two parts: socioeconomic questions, intended to characterize the participants; and five open-ended questions, designed to explore in depth the lived experience and the meanings attributed to care and the perceived barriers.
The interviews were recorded on tablets and later anonymized. The researchers applied the principle of theoretical saturation, which was defined as the point at which data collection no longer yielded new insights or themes, thereby not altering the comprehension of the phenomenon under investigation25,26. Saturation allows the focus to remain on the depth and density of experiences, rather than on numerical representativeness, ensuring methodological rigor and coherence. Thus, for both CHWs and patients with type 2 diabetes at different stages, data collection was finalized when the data began to show redundancy, without the emergence of new meanings, according to Fontanella et al27 and Teixeira28.
All stages of the research, including interviews with individuals with type 2 diabetes, were conducted entirely in Portuguese. Although the study was carried out in the interior of Amazonas, we did not work with populations that used specific dialects or languages other than Portuguese. Therefore, the interviewers did not need to be bilingual, and there was no translation process, since all participants understood and communicated adequately in Portuguese.
Data collection was conducted by a trained research team, TMRL Ueno and EB de Leon, who led the World Café and semi-structured interviews. TMRL Ueno, a woman, is a postdoctoral fellow and a tenured professor in the Nursing Program at the Amazonas State University in Manaus, Amazonas. EB de Leon, also a woman, is the coordinator of the matrix project, holds a postdoctoral degree, and is a professor in the physiotherapy program at the Federal University of Amazonas in Manaus, Amazonas. Both researchers have extensive experience in qualitative research and data representation through thematic networks.
Data analysis
The interview transcripts were created using the Reshape® application, which allowed for the initial generation of audio files in text format. All transcripts were subsequently read, reread, and manually checked by the team to ensure accuracy and fidelity to the original content. The English translation was performed exclusively by the project coordinator, a professional fluent in English, guaranteeing the preservation of the essential meanings and nuances of the accounts.
After the coding was carried out to identify patterns in the initial coding and to determine the themes29, the Thematic Network of Barriers and Facilitators for Adherence to Physical Activity Practice was created30.
In the thematic network, responses were visually represented using a coding strategy in which the thickness of connecting lines corresponds to code frequency. Thicker lines indicate greater recurrence of specific codes in participants’ reports, thereby allowing the visualization of the relative prominence of themes within the dataset30. The ecological model was used to guide data collection, analysis, and message development31.
The ecological model described by Whittemore et al was used exclusively as a supporting framework for data analysis32, and not to guide data collection. The analysis itself was conducted through thematic network analysis, allowing for the inductive identification of generating themes. The ecological framework served to guide the interpretative organization of the findings, offering a conceptual direction, as recommended in qualitative studies, in which themes can emerge inductively or be subsequently aligned with theoretical frameworks. Although the ecological model contemplates multiple levels, the data produced by the participants converged on three main axes: intrapersonal, interpersonal, and environmental factors. The third of these grouped institutional, community, and public policy-related aspects, which in practice proved to be intertwined in the lived experience of the participants. Thus, the choice of three levels reflected the emerging thematic structure of the data, maintaining coherence with the phenomenological and interpretative nature of the study. Therefore, the framework of Whittemore et al was used as interpretative support32, while the final definition of the generating themes was guided by the empirical content and the logic of qualitative analysis.
To ensure the validity and reliability of the qualitative study, the guidelines of Lincoln and Guba were rigorously followed33, including the criteria of credibility, transferability, confirmability, and dependability, in addition to the use of the COREQ checklist, to guide the reporting. Credibility was reinforced by the triangulation of sources (CHWs and individuals with type 2 diabetes), methods (World Café and interviews), and interviewer training, with transcripts reviewed and repeatedly read. Transferability was ensured by the dense description of the context (six PHC units in Iranduba) and the characteristics of the participants. Confirmability was maintained through the audit trail (records of decisions and internal checks) and the phenomenological theoretical framework, aiming for interpretative neutrality. Finally, dependability was guaranteed by the standardization of data collection and analysis procedures, consistent training, and documentation of all stages, making the process traceable.
Ethics approval
The study was based on ethical principles from Resolution No. 466/2012 and Resolution No. 510/2016 of the Brazilian National Commission of Ethics in Research of the Ministry of Health. The macro research project had approval from the Federal University of Amazonas Research Ethics Committee (No. 5.931.419). The Municipal Secretary of Iranduba also consented by consent letter. All participants signed the Free and Informed Consent Term and the Authorization Term for the Use of Image and Voice. Participants were identified as A1 to A17 for the CHW, US1 to US32 for the participants who attended the World Café, and U1 to U15 for the participants who participated in the semi-structured interviews to maintain anonymity.
Results
The study involved 64 participants: 47 with type 2 diabetes and 17 CHWs. Of these, 32 participants and 17 CHWs participated in the Prosa e Café dynamic, and the other 15 participants with type 2 diabetes participated in the semi-structured interview. Females constituted most of the sample, representing 81.25% (n=52) of the sample, and participants were aged between 30 and 79 years. A total of 26 participants reported a family income between one and three minimum wages, which is considered low-income (Fig1).
The study results were structured on 27 basic themes for barriers and 20 basic themes for facilitators. These were identified and reorganized into three organizational themes: intrapersonal factors, interpersonal factors, and environmental factors. The grouping of the organizational themes culminated in the overarching theme ‘barriers and facilitators for adherence to physical exercise’, where the thematic network synthesizes the difficulties and facilitators that participants with type 2 diabetes experience in adhering to physical activity from different perspectives of participants and professionals living in a city in the interior of Amazonas (Fig2).
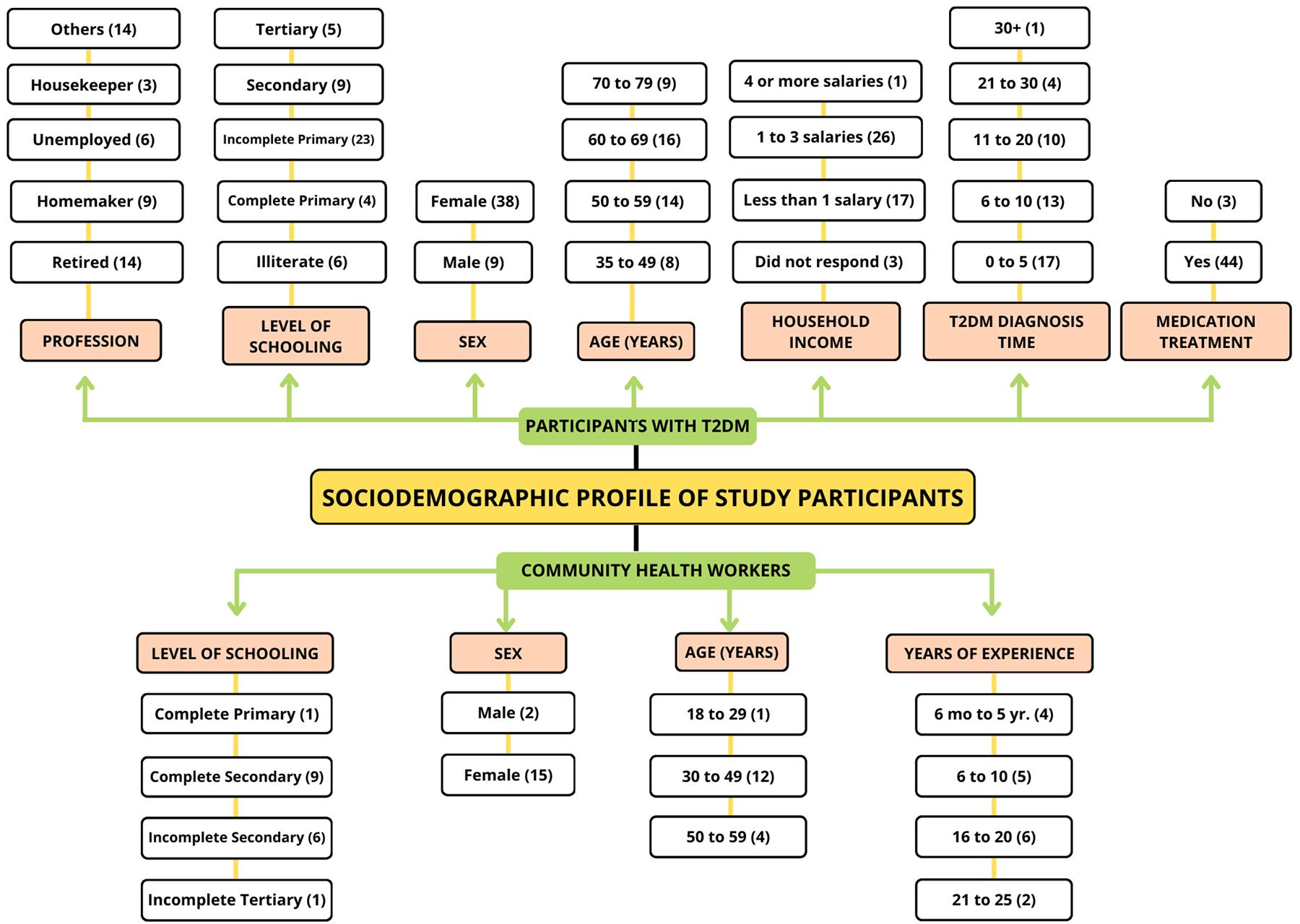 Figure 1: Sociodemographic characteristics of research participants. T2DM, type 2 diabetes mellitus.
Figure 1: Sociodemographic characteristics of research participants. T2DM, type 2 diabetes mellitus.
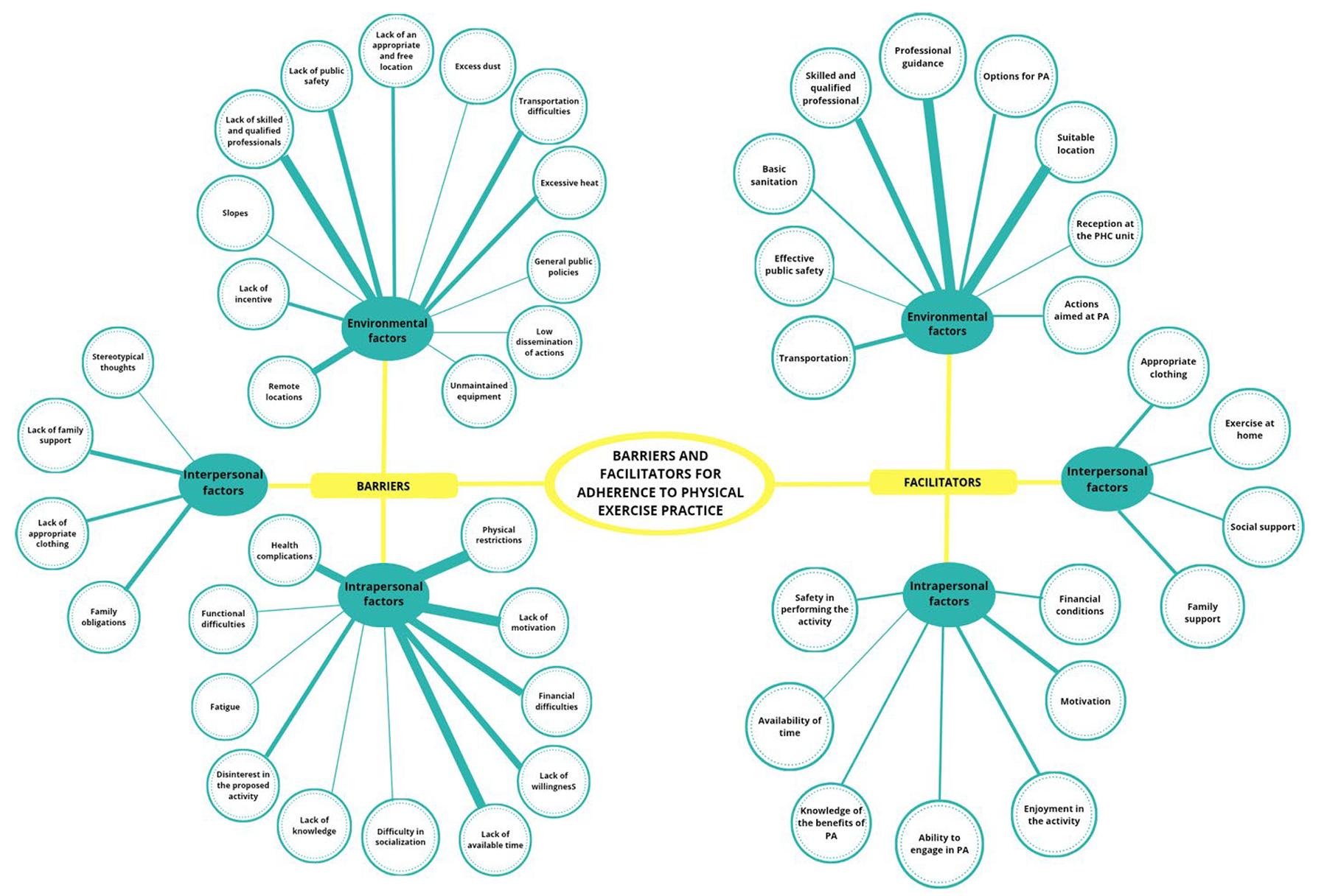 Figure 2: Structure of the Prosa e Café thematic network – barriers and facilitators. PA, physical activity. PHC, primary health care.
Figure 2: Structure of the Prosa e Café thematic network – barriers and facilitators. PA, physical activity. PHC, primary health care.
Barriers for adherence to physical activity practices
Environmental factors
Twelve basic factors described how environmental and socioeconomic conditions affect the adherence to physical activity among participants with type 2 diabetes in the community. These include a lack of qualified and trained professionals, a lack of public safety, long distances to physical activity locations, and excessive heat.
So, what is needed is more physical education professionals to meet the demand we have from patients with hypertension and diabetes. (CHW 4)
It was mentioned about safety. I don’t go out because I only have time at night, and it’s dangerous to leave the house at night. So, public safety today also becomes a factor that contributes to people not seeking a better quality of life. (T2DM interviewee 5)
There is a lot of dust where I live, and it’s not good for walking. (T2DM interviewee 30)
The heat makes me feel unmotivated. When I try to do my things, I feel very anxious! Very irritated! (World Café participant 9)
Intrapersonal factors
Eleven basic factors described the intrinsic barriers that participants with type 2 diabetes face when regularly engaging in physical activity, considering both the patients’ perspectives and those of the CHWs. These barriers are multifactorial, including financial hardship, physical and clinical conditions, insufficient time and motivation, inadequate knowledge, and disinterest in engaging in the recommended physical activity.
So, one of the colleagues said she would like to have a specific person for her; in this case, a personal trainer and a personal trainer is expensive nowadays. I am from the field of physical education, and I know it costs a lot. So, the difficulty is really financial, even when buying a pair of sneakers. And we know that not just any sneakers will do for physical activity. (T2DM interviewee 5)
I feel lazy. I even wake up early to accompany the girls until they catch the bus. I could take advantage of that moment and go for a walk. However, I really do feel lazy. I don’t have a nice answer for that. (World Café participant 6)
The patients do not know the importance of physical activity, and that is why they do not motivate themselves to engage in any physical activity; they lack this awareness. (CHW 14)
Interpersonal factors
Within these four basic factors, participants reported how interpersonal relationships affect the regular practice of physical activity. These behaviors are related specially to family obligations, lack of family support, and surprisingly, the lack of appropriate clothing.
I can’t do it; I need to take care of an elderly person I have at home, I need to take care of my child, and I need to look after my grandchild so that my son can go to work. (US6)
I think what’s missing is family encouragement because we always invite the elderly to participate in the activities. (CHW 2)
It’s just that I don’t stop; my husband gets mad at me because I don’t stop! I wash clothes, I do all the things in my house, thank God, it’s just me. I have some time when I make my lunch, finish eating, then take a shower, lie down, take a nap, and when I wake up, I sit outside. It’s a challenge to walk because, by the end of the day, I’m tired from the routine. (World Café participant 9)
Facilitators to adherence to physical activity practices
Environmental factors
Interactions with the environment and external surroundings facilitate adherence to regular physical activity. In this theme comprising nine factors, participants reported adequate locations for physical activity within the coverage area of the PHC units, professional guidance, and the presence of trained and qualified professionals, among other things.
… there are people who, in the place where they live, do not have an adequate location, so it would help if there were an appropriate place near PHC. (T2DM interviewee 2)
Here in the neighborhood, I haven’t found any available place to do physical activity; everything is far away. It would also help if there were a place like that. (World Café participant 10)
The ease is my guidance to participate in a group called Vida Ativa that is near PHC. (A4)
It would help if there were more promotions about physical activity locations emphasizing that they are free. (CHW 7)
Intrapersonal factors
These seven basic factors describe the individual characteristics influencing a person’s adherence to physical activity. These characteristics are related to financial conditions, personal motivation, enjoyment of the activity, and knowledge of the benefits of physical activity.
What makes it easier to engage in physical activity is the motivation to get better, undergo this surgery, face what needs to be faced, remove the colostomy bag, and return to my normal life. (World Café participant 5)
I think everything is a matter of wanting, right? If you want it and commit to it in your life, you can achieve it. So I believe that since I have this desire to be free from diabetes … I try to do my exercises little by little. (World Café participant 10)
It is very important for us to inform our patients about the benefits of physical activity and to raise their awareness on the subject. If they had a basic understanding of its importance, they would have been practicing it a long time ago … (CHW 7)
Interpersonal factors
These four basic factors refer to how interactions between people facilitate adherence to physical activity. These behaviors are related to social support, family support, the use of appropriate clothing, and the possibility of performing exercises at home.
What makes it easier for all of you who have gone through the [World Café] table[s] is having appropriate footwear and clothing for physical activity. (T2DM interviewee 2)
Sometimes the CHW, nurse, or doctor advised me to do exercises at home, so this makes it easier for me because I don’t need to leave the house [when there are] safety [issues] and dust … (T2DM interviewee 10)
There are weeks when we go for a walk two or three times, and when I go, my wife accompanies me. (World Café participant 4)
Discussion
This qualitative study allows for identifying ideas about the participants’ perceptions regarding the practice of physical activity in a vulnerable scenario. The significant statements from participants revealed important factors that influence both directly and indirectly the adoption of this healthy habit. These reports were important as the first step before implementing the programs aimed at offering actions that promote behavioral change towards adequate levels of physical activity. Similar studies observed that the low education level of participants with type 2 diabetes could significantly affect their knowledge about health care and their pursuit of specialized assistance, directly impacting their quality of life34,35 and healthy behaviors.
Despite clear evidence that physical activity is a key element in the control and management of type 2 diabetes, individuals with diabetes are among the least likely to engage in regular physical activity, and adherence to physical activity is surprisingly low36. Regular physical activity engagement remains notably low among American adults with type 2 diabetes or those at high risk for the disease, with participation rates substantially below public health guidelines37.
Barriers to adherence to physical activity practice
Environmental factors
The factors ‘excess dust’ and ‘excessive heat’ reflect the particularity of the study region. Dust is present in areas without pavement. The characteristics of the built environment play a vital role in determining physical activity behaviors38. Also, the availability of quality walking infrastructure promotes physical activity practice among populations39.
In 2023, Amazonas faced a severe summer, resulting in the most significant historical drought up to that year; this change occurred due to anthropogenic actions that destabilized the environment. Climate change is drastically altering environmental patterns, which directly impacts physical activity habits. Individuals in situations of social inequality are the most disadvantaged as they face greater obstacles to maintaining safe levels of physical activity in the context of these new environmental challenges40. Global warming made the drought that hit the region 30 times more likely, and the increase in temperatures affected the intensity and extent of the episode41. Our reports pointed out excessive heat as a discouraging factor for the practice of physical activity. This factor stands out as one of the region’s main particularities.
The distance from physical activity locations, lack of an appropriate place within the PHC coverage area, poorly maintained physical activity equipment, and lack of public safety – which highlight the disinterest of public authorities in implementing public policies – were also mentioned. These factors hinder participants’ adherence to the practice of physical activity due to the lack of attractive and safe activities close to their residences42-45.
Intrapersonal factors
Physical restriction was the main barrier reported by participants in this study, and it was noted that participants experience arthralgia, which keeps them from practicing physical activity. Feeling this kind of discomfort makes it almost impossible for individuals, especially those with low education and entrenched thoughts about physical activity, to have any desire to practice it46.
Participants also reported lack of knowledge as a factor hindering adherence to physical activity. Limited knowledge regarding the relationship between health and physical activity is a significant factor contributing to physical inactivity. This lack of understanding leads many individuals to underestimate the importance of exercise, often perceiving it as unnecessary47. The lack of or limited knowledge of the relationship between physical activity and health is a relevant factor for physical inactivity7,42. The global increase in the prevalence of type 2 diabetes makes the assessment of knowledge, attitudes, and practices of type 2 diabetes essential to guide behavioral change in people with type 2 diabetes, with knowledge being a prerequisite for health behavior change. The lack of knowledge can also be related to the lack of qualified and trained health professionals18. The presence of a physical education professional in PHC is one strategy to increase the practice of physical activity in the population and minimize the risks of physical inactivity43,48.
Participants also mentioned a lack of motivation. Demotivation for physical activity increases the risk of long-term complications of type 2 diabetes44,49,50. A lack of motivation may stem from two primary factors51. One is an individual’s insufficient motivation to exercise, often due to a limited appreciation of its benefits or not prioritizing it52. The second factor relates to low self-efficacy, as some individuals may feel physically unprepared or believe they lack the skills required to participate in physical activity. Existing health conditions may further hinder their engagement53. Also, lack of time was reported by many, due to a fast-paced daily life resulting from work activities, whether domestic or outside the home environment43.
Disinterest in the proposed physical activity was also a recurring theme in participants’ statements. Several individuals expressed apathy toward attending the gym and performing the prescribed exercise routines. Apathy may be related to a lack of perceived value in physical activity importance or from the belief that the activity will not bring the expected results45,54. In a study by Kang et al, participants reported feeling apathy towards physical activity due to a lack of energy, desire, or laziness45.
Financial difficulties and a lack of qualified and specialized professionals are intrapersonal factors related to the health system55. The cost of accessing physical education and physiotherapy professionals is high, and these professionals should further improve their curriculum to incorporate physical activity, ensuring the availability of structured exercise resources and addressing physical activity misconceptions in PHC settings. Appropriate clothing (or lack of it) was also considered a barrier/facilitator of physical activity adherence, but no other study found a similar factor. This may be because this factor is also associated with financial conditions, given that participants in our study reported not having the financial means to purchase appropriate clothing and that access to such clothing both hinders and facilitates physical activity adherence.
Interpersonal factors
Participants mentioned family obligations as the most prominent interpersonal aspect. People with type 2 diabetes could feel overwhelmed or frustrated in the biopsychosocial context of the disease, and the exhaustion resulting from stress can lead to renunciation or lack of adherence when a person chooses to give up everything, including treatment56, especially in a socially and economically vulnerable setting. Many individuals already do manual labor in their daily activities, such as taking care of household chores or having jobs requiring various movements47.
Lack of social support and lack of family support were barriers to adherence to the practice of physical activity. Without external encouragement from social and family members, it is not easy to maintain continuity in activities45. These two factors were present in our study, and cited in other studies42,43,48,54,55, highlighting that lack of family and social support is independent of region or country.
Facilitators for adherence to physical activity practice
Environmental factors
The factor of ‘suitable location’ was the most frequently cited among the participants’ reports. According to them, it would be of great importance to have a physical activity location close to their homes, making it more feasible to perform exercises. In addition, the participants mentioned that proper professional guidance is essential for the possible independent performance of exercises, according to what is advised. This would be facilitated if there were a physical education professional in the PHC unit57.
When professional guidance is well conducted, it respects an individual’s autonomy and values their potential, increasing the possibility of behavior changes and a consequent improvement in their quality of life58. Recommending physical activity during healthcare appointments by professionals working in PHC units has shown the importance of this guidance in educating and stimulating behavioral changes in people59. This highlights the importance of having a trained and qualified professional in the PHC unit to put these strategies into practice42,58,59.
Intrapersonal factors
Motivation and enjoyment were mentioned by participants as both a barrier and a facilitator, highlighting the importance of the theme. Motivation is the strongest predictor of success in increasing physical activity60. Motivation of individuals with type 2 diabetes to engage in physical activity may be related to various factors, such as progressive improvements in clinical conditions, including weight loss and decreased medication use, as well as the sense of wellbeing and socialization promoted by these activities47.
The participants also described the factors of activity enjoyment and options for physical activity, which complement each other to encourage a more active lifestyle. Some studies emphasize that the enjoyment of physical activity is often associated with the choice of activities that fit personal preferences and provide a sense of achievement, relaxation, or satisfaction6,8,44,61. Finding an activity the participants truly enjoy can transform exercise from an obligation into a pleasurable and rewarding part of their routine.
Participants also cited financial conditions as an essential facilitator for adherence to physical activity. A more favorable economic situation can facilitate physical activity due to better living conditions and access to resources that promote health62.
Interpersonal aspects
Family and friends significantly impact adherence to physical activity and have been classified as facilitating factors in many studies6,7,42,43,49,63. Social and family support is critical in this process due to the possibility of exchanging experiences and constant encouragement63.
The factor ‘appropriate clothing’ was also considered a facilitator for adherence to physical activity; however, no other study has identified such a factor. The ‘appropriate clothing’ factor can be associated with financial conditions, given that the participants in our study reported not having the financial means to purchase suitable clothing and that access to such clothing would facilitate adherence to physical activity.
Knowledge of the benefits of physical activity is an essential facilitator for adherence to practice, providing a greater capacity to engage in it. The authors emphasized that individuals with type 2 diabetes develop positive attitudes toward engaging in physical activity when they have higher levels of knowledge, primarily gained through counseling from specialized professionals about the benefits of physical activity64.
Conclusion
The statements obtained in this research enabled an understanding of the barriers and facilitators that influence adherence to physical activity practice among participants with type 2 diabetes who attended PHC in the Brazilian Amazon. The main barriers were related to financial limitations, physical restrictions, lack of family support, and adverse environmental conditions, such as insecurity and excessive heat.
Identified facilitators, such as personal motivation, family support, and the availability of suitable locations for physical activity practice, reveal that, despite the difficulties, there are elements that can be enhanced to promote greater adherence to physical activity. The presence of physical education professionals in the PHC and adequate support also proved crucial in encouraging physical activity practice, suggesting the need for public policies that integrate physical health and social wellbeing.
Although the presence of a physical education professional is fundamental for adherence to and safety in physical activity, it is equally vital that other health professionals encourage this practice. This need is further accentuated by the lack of assistance in the Brazilian Amazon region, where many communities in remote areas lack specialized professionals due to the scarcity of resources to meet the demand.
These findings may contribute to the development of new research aimed at improving health promotion programs that use behavior change as a central pillar. Behavior change programs for physical activity are promising for improving the health of the population using PHC in Brazil, especially in vulnerable settings.
Limitations
One of the main limitations of this study is its geographic focus, as it was conducted exclusively in a single city in the state of Amazonas, Brazil. This limitation may compromise the applicability of the findings to other locations. However, previous research in the region indicates that various cities in Amazonas share similar demographic and social characteristics. Additionally, adopting a qualitative approach in a low-income population presents significant challenges. Participants may feel distrust or hesitate to reveal personal information, especially if they are unsure how their data will be used or if they have had negative experiences with institutions in the past. Furthermore, low literacy levels and communication difficulties may hinder individuals’ understanding and participation in interviews or focus groups, particularly when discussing complex or unfamiliar topics.
Funding
Fundação de Amparo à Pesquisa do Estado do Amazonas (FAPEAM – Chamada FAP/CnPQ 003/2022), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CnPQ) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES – 001) supported the research.
Conflicts of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
AI disclosure statement
During the preparation of this work, the authors used the Gemini and Grammarly tools to improve the grammar and readability of the English text. After using this tool/service, the authors revised and edited the content as needed and assume full responsibility for the content of the publication.
References
You might also be interested in:
2012 - Delivering free healthcare to rural Central Appalachia population: the case of the Health Wagon