




Introduction
The selection of medical students remains a contentious topic1,2. For decades, medical schools have debated appropriate ways to select the future workforce3. Workforce maldistribution is a significant issue worldwide. The selection approach contributes to the maldistribution in most contexts4. Empirical research and reviews on selection mostly originate from high-income countries5,6.
Limited resources create challenges in translating evidence into practice in low- and middle-income countries (LMICs)7. Selecting students from a large pool of applicants is a complex process3,8. Amid selection debates, medical educators have proposed frameworks and shared experiences to support schools9-13. Applying a standard admission strategy across different contexts is difficult due to varying school missions, differing policy agendas, unresolved controversies, and a lack of consensus14.
Strasser and Neusy (2010) highlighted that context is critical when selecting the future health workforce4. Most schools select students based on academic merit, resulting in the selection of a narrow range of advantaged students. Medical schools in the US, Canada, Europe, and Australia, for example, have adopted strategies to address their workforce needs6,15. Some schools have included socioeconomic status, demographic attributes, rurality of schools and value-based recruitment16,17.
Value-based recruitment aligns with organizational values such as compassion, respect and dignity. Selection based on academic scores only may not achieve a sustainable future workforce18,19. Some schools have incorporated approaches in addition to academic criteria to suit their purposes, with some success20-24. It has been well argued that medical school admissions and selection require a holistic review to ensure that the approaches are driven by evidence, are mission-based and designed with student diversity in mind25.
Reviews on medical student selection heavily focus on ideal selection methods. As a consequence, selections are driven towards academic performance26,27. The reviews also delve into the ability of testing methods to predict success in medical training28-32. Reported selection approaches that focus on ideal methods of selection assume that medical programs are lengthy and require a certain level of cognitive skills33. While methods to recruit for success in the medical course are important, a future-focused approach that addresses the workforce and community health needs is more critical.
Selection processes in developing countries may not be fit-for-purpose; that is, they might not lead to training the health workforce to meet the needs and priorities of communities34,35. The adoption of practices from high-income countries without adaptation to LMIC settings could pose practical challenges. The lack of support, guidance and urgency to apply evidence to practice has stalled the application of research findings in medical schools36. A major barrier to implementing research findings is the uncertainty in defining what institutions look for when selecting potential students36. Current selection approaches often do not address the peculiar circumstances that the most ‘disadvantaged’ medical schools face in LMICs35,37.
There has been a recent shift in the focus of selection to the social accountability of medical schools and their graduates23,38-41. Over the past decade, some institutions have adopted a sustainable selection strategy that extends beyond academic success in the course, aligning with recommendations from the Global Consensus for Social Accountability of Medical Schools (2010)42. Some medical schools in Canada, Australia, Africa and other countries align their selection to produce graduates who will address the health needs of the communities they serve23,38,43-45.
The Asia-Pacific region represents more than 60% of the world population, including the world’s two most populous countries: China and India46. About 40% of the East Asia-Pacific LMICs’ population lived in rural areas in 202347. Adequate sanitation and an aging population with chronic diseases have shifted healthcare demands to value prevention and access to continuous care. There is scarce literature from LMICs to guide the implementation of selection strategies to meet the health needs of geographically isolated and under-resourced populations48,49.
This review explores approaches that medical schools in LMICs in the Asia-Pacific region could utilize in their selection strategies. The purpose is to investigate if medical training institutions recruit students to produce graduates who will address the health needs of their communities. Given the potential impact of selection on workforce distribution, retention and population health22,50,51, the outcome of this review could inform the development of alternative selection approaches for medical schools in LMICs.
Four questions were developed to meet the aim of this review:
- What selection strategies are medical schools in LMICs within the Asia-Pacific region using to contribute to a fit-for-purpose workfoce?
- What selection strategies are medical schools in LMICs in the Asia-Pacific region using to address priority workforce needs?
- What factors inform the choice of strategies that medical schools use for student selection?
- To what degree do medical schools consider a fit-for-purpose future workforce during their selection process?
Methods
A scoping review was selected as it enabled wide concepts to be addressed, generated key concepts and identified gaps in the existing literature while using a systematically structured methodology. It allows for flexibility in including qualitative, quantitative, mixed-methods studies, including the grey literature.
This review followed the methodology outlined by Arksey and O’Malley52 with revisions by Levac et al53 and further enhancement by Daudt and colleagues54. This approach was selected due to the exploratory and descriptive nature of the study objectives. A draft protocol was developed and refined using the Joanna Briggs Institute framework and feedback from co-authors55.
The following steps were taken: (1) identifying the research question, (2) searching for the relevant studies that meet the objectives, (3) selecting the most eligible studies, (4) extracting results and (5) organizing and summarizing the results. The PRISMA Extension for Scoping Reviews (PRISMA-ScR) checklist and guidelines were used to direct the reporting for this scoping review (Supplementary table 1)56.
Elements of the search strategy used to answer the review questions are shown in Table 1.
Table 1: Elements of the search strategy
| Study population | Concept | Context | Outcomes |
|---|---|---|---|
|
Medical students Medical graduates |
Selection | Developing countries | Health workforce |
| Recruitment | Low and middle-income countries | Fit-for-purpose | |
| Admission | Asia-Pacific region | Medical workforce | |
| Matriculation | Doctors/physicians | ||
| Medical graduates |
Literature search
Five electronic databases, relevant websites and grey literature were searched. Scopus, Emcare, Ovid MEDLINE, ERIC and CINAHL databases were deemed most relevant after consultation with the university librarian and the co-authors. The search was focused or broadened using truncation symbols and the Boolean operators ‘AND’ and ‘OR’. The databases were searched using MeSH and keywords with no limits applied. A hand search of landmark empirical research papers on the subject within and outside the Asia-Pacific region was conducted. References of review articles within LMICs were also searched. Backwards and forward citation searching was conducted using a list of key studies identified through the search. References frequently cited by published studies from LMICs and non-LMICs were also searched. Only documents in the English language were eligible for inclusion.
The four main concepts searched were ‘student selection’ AND ‘fit-for-purpose’ AND ‘health workforce’ AND ‘LMICs’. Keywords from published articles were extracted and used in search combinations. In addition, keywords and subject headings were applied to each database to check for synonyms. Synonyms were incorporated during the database trial searches. Multiple trial searches and refinements were carried out between April and June 2024 to evaluate the search results before the final search was executed in July. No date restriction was applied for the reviewed documents.
The final search strategies were formulated after agreement among the authors (Supplementary tables 2–6). A Google Scholar web search was conducted to identify relevant articles that might not have been captured in the database search. A grey literature search was conducted through the James Cook University online library guides website57. Open Access Thesis and Dissertations58, ProQuest Theses and Dissertation database, Advanced Google Scholar search, WorldCat Conference Proceedings Citation Index Social Science & Humanities59, and the National Institutes of Health list of grey literature sources60, like the WHO Western Pacific health workforce website, were searched61. Unpublished theses, policy documents, abstracts of conference materials, technical reports and guidelines were retrieved from the grey literature search.
Study selection
All publications that focused on medical student selection, graduate outcomes and contextualized to LMICs in the Asia-Pacific region were selected. Further refinements using the inclusion criteria were carried out in the final step of the selection process. A PRISMA set-up was created using EndNote to manage the selection process. The lead author carried out the primary search, title and abstract screening using the inclusion and exclusion criteria (Table 2). Five other team members worked independently and collaboratively to assess the elligibility of relevant studies. Three were very senior medical education experts, one a senior dental educator, and a senior research fellow with expertise in health systems and medical education. Relevant publications were exported from EndNote and summarized in Microsoft Excel for analysis. The summary of selected publications, as outlined in Table 3, was shared with all the co-authors for independent review.
Table 2: Inclusion and exclusion criteria
| Criterion | Inclusion | Exclusion |
|---|---|---|
| Study focus | The selection of medical students is closely connected to graduate outcomes and the priorities of the country | The selection method is not linked to graduate outcomes and health priorities |
| Population | Medical graduates | |
| Journal quality control | Peer-reviewed | |
| Type of article | Primary research articles | Reviews, editorials, opinions, book reviews, letters to the editor, commentaries or where full text was not available |
| Context | Low and middle-income countries within the Asia-Pacific region, including all eight countries in South Asia | High-income countries and/or outside the Asia-Pacific. Non-English language publications |
| Study type | Quantitative, qualitative and mixed-methods studies | |
| Grey literature | Non-research sources, policy documents, unpublished theses or dissertations | |
| Time period | No restrictions | |
| Language | Publications in the English language only |
Quality appraisal
The Quality Assessment Tool for Studies with Diverse Designs (QATSDD) was used due to anticipated variability in studies, and demonstrable reliability and validity in the appraisal of diverse qualitative and quantitative studies62. Each study was scored using the 16-item criteria with a maximum score of 42 points. No publications were excluded from the review after the QATSDD scores were allocated. Identified strengths and weaknesses were considered in the synthesis of themes and discussion.
Ethics statements
Eleven (69%) studies had explicit ethics approval statements documented and five (31%) did not have any documention. The five studies used school administrative data and graduate records that might have been covered under some other instituional approval processes.
Analysis
Data extracted from selected studies were deductively coded using a pre-set framework (Table 4) to answer the three guiding questions for this review. Subsequent inductive coding was manually conducted to create themes from the 16 included studies. A narrative synthesis was carried out using the derived themes.
Ethics approval
Ethics approval was not required because the method involved collecting, analyzing and synthesizing publicly available data.
Results
Database search results
The search results are highlighted in the PRISMA flow chart in Figure 1. Database searches yielded 5045 published studies. A total of 3649 publications were subjected to title and abstract review after duplicates were removed. Out of the 1252 full-text publications eligible for review, 1242 did not meet the inclusion criteria. Ten publications were extracted for detailed review.
Excluded studies consisted of non-empirical research related to selection tools, studies not linked to graduate outcomes, selection and in-course performance, non-Asia-Pacific or non-LMICs content, and those that did not focus on the objectives of the review. The context criterion excluded most studies.
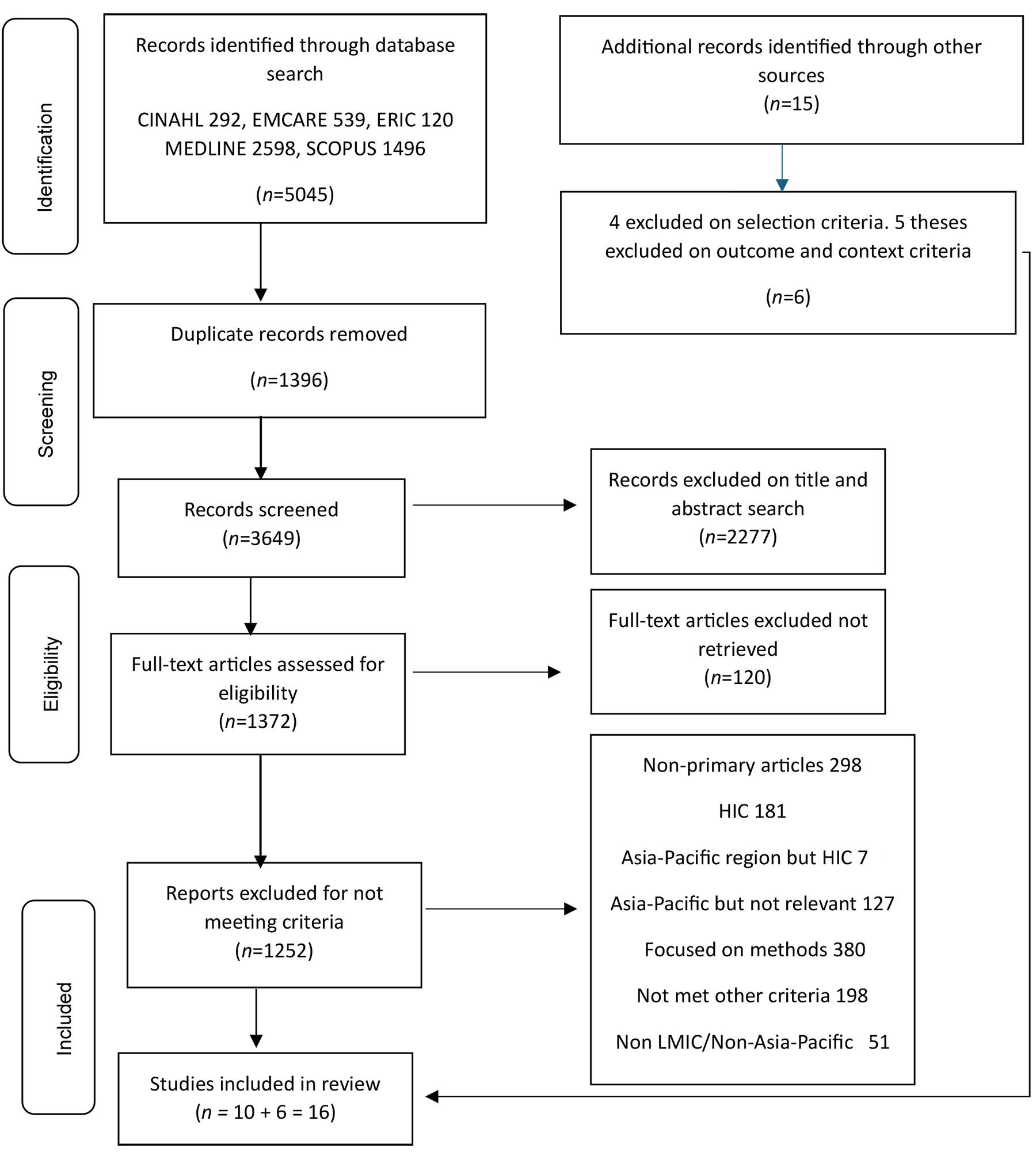 Figure 1: Flow chart of the literature search using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) template. LMIC, low- to middle-income country. HIC, high-income country.
Figure 1: Flow chart of the literature search using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) template. LMIC, low- to middle-income country. HIC, high-income country.
Additional studies identified
Fifteen published studies were retrieved from hand searches of reviews and primary articles. Five publications were excluded on outcome and context criteria, and another four did not focus on the outcome criteria. Six studies were included for review.
Grey literature search
Five theses on medical student selection were obtained. They were excluded on context and outcome criteria. A study titled ‘Doctors for the Barrios’ from the Philippines63 was excluded because it had a different focus.
Description of studies
A total of 16 studies were eligible for review and are summarized in Table 3. Studies were set in China (n=4), Thailand (n=4), the Philippines (n=3), Indonesia (n=2), Nepal (n=2), and Taiwan (n=1). Ten were cross-sectional studies, four were retrospective, one was a cohort study and one was an exploratory study. All the studies used quantitative methodologies.
Table 3: Summary of published studies, in chronological order (N=16)22,24,50,51,64-75
| Author(s), year | Title | Country | Aims | Study design and methodology | Summary of findings |
QATSDD score (%) |
|---|---|---|---|---|---|---|
| Wang, 200264 | A comparison of metropolitan and rural medical schools in China: which schools provide rural physicians? | China | To characterize some of the rural medical schools and compare them with metropolitan medical schools in the provision of rural physicians. | Cross-sectional survey, between 1 and 20 April 2001, of 12 randomly selected rural schools and 12 metropolitan medical schools (six affiliated to the Ministry of Health and six to provincial governments). Conducted questionnaires and internet searches on the official websites of selected schools to gather information. Variables were compared between the rural and metropolitan schools using an analysis of variance test. | The metropolitan schools had 893±117 graduates. Rural schools produced 258±86 graduates. All rural medical schools produced rural physicians. Only 73 graduates from the 12 metropolitan schools entered rural practice – fewer than the number produced by one rural school. Factors such as rural location, enrolling students of rural backgrounds and a government-regulated employment policy enabled rural schools to provide rural physicians. |
26 |
| Cristobal and Worley 201250 | Can medical education in poor rural areas be cost-effective and sustainable: the case of the Ateneo de Zamboanga University School of Medicine | Philippines | To examine the hypothesis that a medical school in a low-resource setting, based on volunteer faculty, can be sustainable and associated with improvement in the medical workforce and population health outcomes. | Retrospective study of graduates’ destination. Descriptive analysis looking at the graduates’ destinations since the establishment of ADZU. Intervention since graduates were produced as measured by the infant mortality rate and community improvement was described. | Since the first 15 graduates of ADZU in 1999, by 2011, more than 160 students had successfully graduated. 80% of graduates practiced in the local underserved regions during the study period. Adopting a socially accountable approach to medical education produced doctors who improved service in underserved regions. There was a 55% increase in municipalities with a doctor, a decrease in the infant mortality rate of almost 90% compared to the national rate of 50% since 1994, when the school was set up. |
57 |
| Zimmerman et al, 201265 | Medical students’ characteristics as predictors of career practice location: retrospective cohort study tracking graduates of Nepal’s first medical college | Nepal | To determine which characteristics of medical students are associated with graduate doctors staying to practice in Nepal or its rural areas. | Retrospective cohort study. Data collection over 24 months in three phases. Review of records at the Institute of Medicine Nepal, a written questionnaire from graduates and reporting by classmates. Involvement of alumni networks. 710 graduates from the first 22 years (1983–2004) of Nepal’s Medical College. Place of birth, high school attended, sex, pre-medical education, year of graduation, final academic scores, age at matriculation and location of practice were analyzed. Logistic regression analysis and odds ratio for the likelihood of remaining in Nepal or working in rural districts. | Medical student characteristics such as paramedical background, rural birthplace, and lower academic rank in medical school class were associated with a doctor remaining in Nepal. The same characteristics were associated with a doctor working outside the capital city of Kathmandu. |
55 |
| Putthasri et al, 201366 | Thailand special recruitment track of medical students: a series of annual cross-sectional surveys on the new graduates between 2010 and 2012 | Thailand | To compare the graduates of the CPIRD and ODOD graduates with graduates of the normal track on their rural attitudes, intention to fulfil the 3-year mandatory service and competency. | Cross-sectional survey. Self-administered questionnaire to 4703 graduates for three consecutive years from 2010 to 2012 in Thailand. Surveys on demographics, mode of admission, medical school location, residence for 1–15 years, current residence, secondary school, parents’ education profile, attitudes to rural practice, 14 medical and public health competencies and intention to complete 3-year mandatory service and plans thereafter. | Graduates of the special program (CPIRD and ODOD) scored higher on rural attitude, had a significantly higher intention to fulfil their 3-year compulsory service, and had higher competencies in domains other than major clinical subjects compared to normal-track graduates. Normal-track graduates had higher competencies in clinical subjects. Normal-track graduates who spent their childhood life in Bangkok, resided in Bangkok and attended secondary school in Bangkok had a significantly lower intention to fulfil their 3-year compulsory service. |
71 |
| Pagaiya et al, 201567 | Rural retention of doctors graduating from the rural medical education project to increase rural doctors in Thailand: a cohort study | Thailand | To examine the impact of the CPIRD on doctor retention in rural areas and public health services. | Cohort study utilizing longitudinal data of graduates between 2000 and 2007. Administrative data from the Ministry of Health information system and collected between June 2000 and July 2011. Kaplan–Meier method of survival analysis and Cox proportional hazards modelling for retention. | CPIRD doctors were more likely to stay longer in rural areas and remain in public service compared to their normal-track counterparts. The trends of rural turnover of doctors were observed to be increasing in both groups, suggesting a review of the recruitment programs. |
62 |
| Arora et al, 201768 | Retention of doctors in rural health services in Thailand: impact of a national collaborative approach | Thailand | To examine the retention in the Ministry of Public Health hospitals of medical doctors who graduated from the special recruitment (CPIRD and ODOD) and normal tracks between 2001 and 2015 and identify factors associated with rural retention over the period. | Retrospective study. Medical graduates who started work for the Ministry of Public Health between 2001 and 2015. Data from ministry records were analyzed for factors associated with retention for at least 3 years in the Ministry of Publich Health. Multiple logistic regression analysis was conducted. | 19,338 graduates. About one-third were CPIRD and ODOD graduates. Retention rates in the Ministry of Public Health were 52% for the normal track and 78% for the special track. 62% of special-track graduates employed in 2001 remained in the ministry. 90% of the special track graduates worked in the provinces to which they were initially assigned. Factors associated with 3-year retention in the Ministry of Public Health were recruitment track, sex and those working in the northern geographical region. |
67 |
| Siega-Sur et al, 201722 | The impact of socially accountable, community-engaged medical education on graduates in the Central Philippines: implications for the global rural medical workforce | Philippines | To describe the impact of socially accountable health professional education on graduates, specifically their motivation towards community-based service, preparation for addressing local priority health issues, career choices, and practice location. | Cross-sectional study. Survey questions on graduates from SHS-Palo and a medical school with a conventional curriculum. Requested information: background (age, gender, gross family income, schooling), undergraduate NMAT score, financial support during medical school, motivation for studying medicine, motivation for selecting their respective school, intentions at the time of graduation (career, rural/urban practice), practice history (attitude to community service, preparedness for practice, current practice discipline, current practice location, current practice facility, length of employment, and specialization. 59% response rate for SHS-Palo and 36% for the conventional school. Bivariate analysis, two-tailed student t-tests, Pearson’s χ2 for trend. | SHS-Palo graduates had significantly more positive attitudes to community service and were more likely to work in rural and remote areas in the district or provincial hospitals or rural, government health services as public health or municipal officers. SHS-Palo graduates also stayed longer in their first medical posting and their current jobs. |
71 |
| Upadhyay et al, 201724 | Admitting deserving medical students from rural and disadvantaged: Patan Academy of Health Sciences approach | Nepal | To describe the innovative medical student selection scheme adopted by PAHS in Nepal for its MBBS program and its initial findings. | Descriptive cross-sectional study. Admission data on medical students recruited in PAHS from 2010 to 2012 using the three-step-based selection scheme. Admission data assessed students’ cognitive attitudes and personalities, followed by an admission objectively structured performance examination and a social inclusion matrix. Descriptive statistics to describe student demographics and scholarships awarded based on the three different scholarship schemes. | 175 students enrolled between 2010 and 2012 at PAHS. More than half of the students were from rural Nepal. 60% of students received different categories of scholarships. Increased students enrolled by the SIM criteria from 0 in 2010 to 5.7% in 2011 and 6.45% in 2012. Balanced selection of the poor, ethnic minorities, and indigenous nationalities. Overall increase in scholarships awarded to those with permanent residence in rural areas over 3 years. The selection scheme enrolled a higher proportion of students from rural and disadvantaged groups. |
52 |
| Techakehakij and Arora 201769 | Rural retention of new medical graduates from the Collaborative Project to Increase Production of Rural Doctors (CPIRD): a 12-year retrospective study | Thailand | To compare the retention of physicians in the Ministry of Public Health hospitals across the tracks of entry, and to examine the probability of 3-year retention among rural physicians from different tracks of entry. | Retrospective study. Data from the Ministry of Public Health’s CPIRD Registry database. New graduates who joined the Ministry of Public Health from January 2003 to October 2014 and followed until June 2015. Tracks of entry, demographics and region of the workplace were compared. Time of entry to resignation date analyzed using Kaplan–Meier survival estimates. Comparison using log–rank test. Cox proportional hazard model to examine tracks of entry to survival from rural service. | 15,253 total physicians graduated in 12 years. 68.7% graduates of the normal track, 26.1% from the regular CPIRD, 3.3% from ODOD, 1.33% from civil servants and 0.4% from non-civil servant graduates. High rural retention of graduates of the CPIRD program compared to graduates of the normal track program. Lower rural resignation and higher 3-year retention were observed in the CPIRD graduates compared to graduates of the normal track. Some variations of rural retention across the different CPIRD tracks, with higher 3-year rural retention rates among the graduate civil servants. 3-year retention probability is not significantly different between CPIRD and ODOD graduates. |
62 |
| Labarda and Labarda, 201851 | A community-based strategy in medical education of the University of the Philippines, Manila-School of Health Sciences – lessons from innovations in human resources for health development in a developing country | Philippines | To examine human resources for health inequity in the Philippines and review the medical school’s performance in terms of addressing human resources for health distribution. | Cross-sectional study. Graduate data generated by the College Secretary’s Office and Dean’s Office from the graduate tracking survey of Manila School of Health Sciences students from 1976 to 2011. Graduates by municipalities and geographical region, socioeconomic characteristics of municipalities, number of health professionals produced (midwives, nurses and physicians), return of service to communities, location of health service delivery and migration. -Descriptive statistics. The Gini coefficient as an index of inequality for inequality in the workforce among regions of the country. | Graduates came from all regions except the National Capital region. 55% of the total admissions came from fourth- and fifth-class municipalities (the highest income is the first class, and the poorest is the sixth class). Students from first- to third-class municipalities comprised 43.2% of total enrolment.1.8% came from the poorest municipalities. After 36 years of work in training health workers for poor and underserved communities in the Philippines, the Manila School of Health Sciences has produced more than 2000 health workers, of which more than 100 are medical doctors. 90% of graduates have stayed in the country. Nearly 60% have continued to serve in their local communities or within nearby environments. About 10% of graduates have migrated. |
52 |
| Liu et al, 201870 | Attitude towards working in rural areas: a cross-sectional survey of rural-oriented tuition-waived medical students in Shaanxi, China | China | To examine the attitudes of rural-oriented tuition-waived medical students in Shaanxi towards working in rural areas and the related influencing factors. | Cross-sectional survey. Email-based self-administered questionnaire that assesses demographic characteristics, policy cognition, policy choice motivation, policy satisfaction, intention to break the contract and intention to remain after the contract expires. Descriptive statistics, univariate analyses, Pearson’s χ2 tests, correlation analysis, multivariate analyses and binary logistic regression analyses. | 232 rural-oriented tuition-waived medical students participated and completed the questionnaire. Almost 93% of rural-oriented tuition-waived medical graduates intended to break working in rural township hospital contracts 6 years after graduation. 13% intended to remain in rural areas, almost 67% had no intention of remaining, and 32% were unsure. Positive factors for working in rural areas are being female, mothers educated at the level of primary school or below, good understanding of the policy, good insight into the value of rural work and satisfaction with the policy. Positive factors for remaining in rural areas were being female, of rural origin, having no regular family monthly income, the father being a farmer, the mother educated up to post-secondary or above, a good understanding of the policy and the value of rural medical work. |
57 |
| Pei et al, 201871 | The selective admission policy of medical undergraduates in Western China: applicants' real attitudes to the choice of a rural medical career | China | To analyze the selective admission policy in western China from the perspective of medical students’ attitudes towards rural career choice. | Cross-sectional survey. Anonymous questionnaire and face-to-face interviews to assess sociodemographic characteristics, western and traditional medicine majors, family background, entrance scores, contributing factors to rural medical career choice, motives for selective admission policies application and attitudes. Descriptive statistics, Inferential statistics: χ2 test for categorical variables of single-factor analysis. Unpaired t-tests or one-way analysis of variance for continuous variables of single-factor analysis. Ordinal stepwise logistic regression for association between independent variables. | Medical undergraduates’ enthusiasm to work in rural areas was very limited in Gansu province, western China. Students’ attitudes and their professional and personal environment were affected by their socioeconomic and cultural status. Intrinsic motivation was of less importance in rural career choice than extrinsic motivation. |
50 |
| Noya et al, 202172 | Factors associated with the rural and remote practice of the medical workforce in the Maluku Islands of Indonesia: a cross-sectional study | Indonesia | To describe factors associated with actual rural and remote practice, preferred rural and remote practice, and intention to remain in practice in Maluku province. | Cross-sectional study. 324 doctors recorded responses, so 79% of eligible participants commenced the survey. 241 (59%) doctors working in the Maluku province completed the survey. Online survey with multiple-choice, dichotomous, multi-response and Likert-type questions. Participant characteristics, location of the workforce, intention to remain in practice in Maluku, and preference for future rural and remote practice in Maluku province were assessed. | A rural medical school (Pattimura University) helps supply doctors to rural and remote regions in Indonesia. A sustainable rural and remote workforce in Maluku province is possible if special attention is given to the recruitment and retention of doctors with a rural background and ongoing support through attractive opportunities to sustain their practices. Stronger and sustained collaborations between medical schools and local government are crucial in the implementation of relevant strategies. |
64 |
| Lin et al, 202173 | Differences in demographics and motivation to study medicine with respect to the medical students’ channel of admission: a national study | Taiwan | To compare the demographic characteristics and motivations for studying medicine of first-year medical students admitted to Taiwanese medical schools through either MMIs or the JCEWT channel. | Cross-sectional survey of seven medical schools. Semi-structured questionnaire. 205 MMI group and 192 JCEWT group (N=397). Response rates varied from 90% to 100% across the seven medical schools. Information on MMI or JCEWT admission channel, gender, location of living (metropolitan or rural), high school type (public or private), parents’ socioeconomic status, and motivations for studying medicine was obtained. Descriptive statistics, Pearson’s χ2 test, Fisher’s exact test, and logistic regression. | Irrespective of the channel of admission, most medical students come from metropolitan areas (80–86%), belonged to high-socioeconomic status families (73–76%), and had mixed motivations (51–96%). Female medical students, private high school leavers, and students who were less motivated by physicians’ socioeconomic status were more likely to be selected through the MMI than the JCEWT channel. |
71 |
| Soemantri et al, 202274 | Evaluation of situational judgment tests in student selection in Indonesia and the impact on diversity issues | Indonesia | To evaluate the use of an SJT for selection and the impact on student diversity relating to gender, ethnicity and socioeconomic status. | Exploratory study. The SJT was piloted in a single institution, the Faculty of Medicine, Universitas Indonesia. Two pilot-year cohorts of student intakes in 2017 and 2018. 2017 (n=446) and 2018 (n=508). Student demographics broken down by gender, socioeconomic status (high school origin and parental educational background) and ethnicity. Mean SJT scores across both years. Independent t-tests for differences between genders. Analysis of variance for differences among other grouping variables. | SJT demonstrated good internal consistency with Cronbach’s alpha of 0.80 and 0.81, respectively. Significant differences in SJT scores based on gender in both years. Females consistently outperformed males. No significant differences in high school origin, parental educational background or ethnicity. |
71 |
| You et al, 202375 | Does medical education reform change who is selected? A national cross-sectional survey from China | China | To examine how policy changes in medical education to improve the quality of doctors, translated into practice. | Cross-sectional survey. The questionnaire was emailed and sent on social media networking platforms. Data were collected from 193 medical schools across China via the 2021 China Medical Student Survey, developed and administered by the National Centre for Health Professions Education Development. National College Entrance Exam, sociodemographic variables, prior academic attainment, pilot program selection, traditional program selection, region, the tier of medical school, geographical region, the orientation of education program and speciality of education programs were obtained. Mann–Whitney U-test for continuous variables. Differences in proportions between groups were analyzed using the χ2 test for categorical variables. Multilevel mixed-effects linear regressions on numerical selection results variables. Multilevel mixed-effects logistic regressions on categorical selection results variables. | 123 out of 193 (63.7%) of medical schools offering undergraduate programs participated. 125 licenced to run PP, of which 76 (60.8%) took part in the survey. 204,817 respondents: 194,163 (94.8%) were in the traditional program and 10,654 (5.2%) in a pilot program. Pilot program respondents had significantly higher National College Entrance Exam scores than their traditional program counterparts, were significantly more likely to come from urban areas, not be first-generation college students, and have parents with higher occupational status and income. |
81 |
ADZU, Ateneo de Zamboanga University School of Medicine. CPIRD, Collaborative Project to Increase Production of Rural Doctors. JCEWT, Joint College Entrance Written Test. MBBS, Bachelor of Medicine, Bachelor of Surgery. MMI, multiple mini-interview. NMAT, National Medical Admission Test. ODOD, One District One Doctor. PAHS, Patan Academy of Health Sciences. QATSDD, Quality Appraisal Tool for Studies with Diverse Designs. SHS-Palo, University of Manila-School of Health Sciences. SJT, situational judgement test.
Quality of included studies
The scores for the individual studies ranged from 26% to 81%, as shown in Table 3. All the studies were included in the narrative synthesis. Descriptions of the study settings and statements of aims and objectives were notable strengths among the selected studies. The sample size of cross-sectional studies was determined by the response rates and was generally satisfactory. Out of the 10 cross-sectional studies, eight (80%) reported response rates ranging from 47 to 99% and two (20%) didn’t report response rates due to the nature of the studies. Among these eight, six studies (75%) achieved rates between 60% and 99%, while the remaining two reported response rates of 47% each.
Data collection procedures, the rationale for the choice of data collection tools and recruitment data were satisfactorily explained in the studies. The justification of analytical methods was good overall, apart from four studies that provided a basic rationale for the applied analytical methods.
Synthesis of findings
The 16 included studies were reviewed, and content was deductively assigned according to the three research questions (Table 4), followed by the inductive generation of five major themes. Similarities were found in the approach to student selection across the region's LMICs.
Table 4: Framework of analysis of medical student selection approach and a fit-for-purpose workforce, by country22,24,50,51,64-75
| Author(s), year | Country and setting | Selection approach and method | Factors informing selection strategy | Fit-for-purpose workforce consideration |
|---|---|---|---|---|
| China | ||||
| Wang, 200264 |
Mainland China. The location and number of rural medical schools are determined by national and local governments. 82 medical schools spread across 31 provinces. 40 schools were defined as rural schools, and the rest of the 42 were metropolitan. 10 rural medical schools and 12 metropolitan medical schools were randomly selected between 1 and 20 April 2001. Graduate employment status in the year 2000 was studied. |
Selection is by a quota system regulated by the Ministry of Education or the provincial government. Rural schools had designated places for rural students, ranging from 9.1% to 15.1% in the study. Metropolitan schools had a lower number of places for rural students, ranging from 1.0% to 6.7%. The selection method was not explained. |
The Ministry of Education's employment policies required graduates to practice at their place of origin. Specific guidelines by the Ministry of Education or provincial governments to schools on the number of enrolments and geographical areas from which they were to select students. Country policy on restriction of rural to urban migration of physicians and the general population. The government's effort to provide the 900 million rural population in China with quality health care. |
Graduates to serve and provide quality health care to China’s huge rural population. A one-off financial grant equivalent to 6 months' salary is offered by a few medical schools as an incentive to graduates who wish to practice in rural counties. |
| Pei et al, 201871 | Western China’s Lanzhou University and Gansu University of Chinese Medicine. Enrolment was from 2010 to 2015. Cluster samples from the Medical College of Lanzhou University and Gansu University of Chinese Medicine. A total of 1133 undergraduates studied. |
Medical undergraduates are chosen under the selective admission policy in Western China. Students majored in western medicine or traditional Chinese medicine under the selective admission policy. Preferential admission to students of rural origins with quota restrictions. Rural students should have household registration in the China population management system and have lived in a rural town, county or village. Students voluntarily apply after completing the Chinese Ministry of Education state examinations. A qualified score will enable entrance to the medical university. Ranked scores determine admission until the quotas are filled. |
The government’s selective admission policy to recruit rural students since 2010. Improve rural township medical services in western China. A huge population reside in the rural mainland, and a small proportion of doctors work in rural areas in China. |
Promote rural medical career choices after graduation. Selection considered the need to improve the rural medical services system in townships in western China. Improvement in basic healthcare coverage and health services towards the grassroots/rural people in China is needed. Some students received full financial support and other benefits during their undergraduate study. Further formal training for rural health work is determined by their contract during their study. In exchange, students work for 6 years in rural communities after graduation. |
| Liu et al, 201870 |
The RTME is one of the health workforce development plans in China. From 2010 to 2017, approximately 43,000 rural-oriented tuition-waived medical students were enrolled. 232 students from the first group enrolled in the RTME program in 2010 at the Xi’an Medical University and Yan’an University in Shaanxi, the western province of China, participated in the study. |
Recruit students from rural areas with a plan to work in township hospitals for 6 years after they graduate. Contractual agreement with the government, provision of living allowance in exchange for tuition waiver. This study focused on rural-oriented tuition-waived medical student attitudes towards working in rural areas and the related influencing factors. No details on student selection methods. |
China’s RTME program since 2010. | Foster the right attitude towards working in rural areas. Address the shortage of rural health workers in the 23 provinces of the west and middle regions in China, where RTME was trialled. |
| You et al, 202375 |
Before 2012, a significant number of doctors had not met international standards of admission. 125 out of 193 medical schools implemented a pilot program in line with the Ministry of Health and Ministry of Education policy to improve the quality of doctors. 204,817 students participated in this study to compare who was selected for the new pilot program and the traditional program. 5.2% were in the pilot program and 94.8% were in the traditional program. |
Schools selected academically strong candidates using the National College Entrance Examination scores for the pilot program. |
Different doctors’ training programs are offered by specialized secondary schools, junior colleges and universities. Different standards of selection and varying standards of practicing doctors. Adherence to the Education Plan for Excellent Doctors policy, developed to improve the quality of medical education under the pilot program and better serve China’s health needs. |
This policy change was implemented to address training gaps and help achieve quality graduates. Quality was defined by high prior academic achievements. A reduction in student diversity because of this policy change. |
| Indonesia | ||||
| Noya et al, 202172 |
This study described factors associated with actual rural and remote practice in Maluku, a remote, underdeveloped and poorly served province in Indonesia. Medical students from Maluku province used to attend schools in urban and city areas in Indonesia before the province had a medical school. Pattimura University Medical School was established by the Indonesian government in 2008. The school selects students from within the region and provinces close to their communities. 410 doctors working in Maluku province participated in the study. |
The first five cohorts of 50 students were partly funded by the government. More than 20% of the first cohort selected were of rural backgrounds. No specific selection method was mentioned. |
Shortage and maldistribution of doctors reduce health service equity in the most rural, remote and poor communities. Building the Pattimura University Medical School in Maluku, close to the underserved communities to avoid travel to Jakarta and other cities for study. The school addressed the selection strategy to include more students of rural backgrounds who lived close to the province’s training institution. |
The intention is to facilitate access by selecting students from nearby areas for graduates to work in rural and remote regions within the province. Improve the number of doctors in the rural and remote province of Maluku to serve the underdeveloped and poorly served islands within the province. Selecting students with a rural background and supporting them through attractive opportunities to stay. |
| Soemantri et al, 202274 | The study was conducted at the Faculty of Medicine, Universitas Indonesia, a state-funded university. Two pilot-year cohorts of student intakes consisting of 446 students in 2017 and 508 in 2018 were selected using the SJT. |
Selection of medical students was not based solely on academic achievements. The non-academic attributes were included. In addition to academic attainment, the SJT was piloted to assess the non-academic attributes of medical students and the impact of using the SJT on student diversity. |
Selection practices changed to include non-academic attributes to align with the Indonesian Medical Education Law Number 20 of 2013. Indonesia’s rich, diverse socio-cultural context, with more than 300 ethnic groups, underscores the need for medical schools to adopt an equitable and fair selection process that encourages broader participation in medical school selection. |
Ensuring fair opportunities for medical students from diverse ethnic groups. Possessing the desirable non-cognitive attributes required of doctors. In addition to professionalism (encompassing moral values and integrity), effective communication and self-awareness were important graduate academic attributes. |
| Nepal | ||||
| Zimmerman et al, 201265 |
Nepal has a population of 28 million. It is a low-income country and struggles with workforce distribution and migration. Nepal’s Institute of Medicine was set up in 1978. The institute’s first 22 graduate classes were tracked for their practice location to determine the characteristics of medical students that were associated with staying to practice in the country or its rural areas as doctors. |
Two pre-medical pathways existed. Initially, the institute selected rural students with paramedical backgrounds. Changed to selecting science students with total classroom training based on entrance exam scores, rather than those with a paramedical background. |
Workforce distribution and migration. The ethos of the medical school is to serve the remote population. |
Staying to practice in Nepal or its rural areas outside the city of Kathmandu and serving the disadvantaged and rural communities. The purpose of selection was more likely to be achieved when those from rural areas with a paramedical background were selected. |
| Upadhyay et al, 201724 |
Medical students recruited into the Patan Academy of Health Sciences in Nepal for the years 2010–2012 inclusive. 60 students enrolled in 2010 and 2011, and 55 students were enrolled in 2012. The study described the academy’s selection approach to improve the selection of rural and disadvantaged groups. |
Patan Academy of Health Sciences purposefully selects students based on a three-step social inclusion matrix approach. The practice positively favored recruitment and scholarships for students from rural and disadvantaged areas from 2010 to 2012. The social inclusion matrix selection criteria are as follows: Stage 1: Applicants’ cognitive skills, as well as personality and attitudinal traits, were assessed using the Personal Quality Assessment tool. The tool had four subsets: the Mental Agility Test; Moral Orientation in Justice and Caring; Narcissism, Aloofness, Confidence and Empathy; and Personal Characteristics Inventory. Stage 2: Admission Objective Structured Performance Examination. Satisfactory performers progress to the next stage. Stage 3: Social inclusion matrix variables were gender, caste/ethnicity, remoteness (rurality), community or public school background, applicants’ rural health work experience and the Human Development Index status of their place of permanent residence. Eligibility for any of the three scholarship schemes was based on the combinations of the three-step selection outcome. Decisions on self-funded students were based on the first two stages only. |
Aligning with scholarship awards policy. The scholarship schemes were ‘partial’, ‘full’’ and 'collaborative'. The partial scholarship had a 50% benefit in tuition fees while the other two were fully funded. The collaborative scheme was co-funded between the government and rural communities. Non-academic attributes were recognized in the selection of future doctors. Preferential credits were granted based on students’ socioeconomic backgrounds to ensure that those from disadvantaged communities received scholarships. |
Service to the rural, remote and disadvantaged segments of Nepal’s society. Consideration for students of low socioeconomic status, from rural and disadvantaged communities to access medical schools and contribute some years of service back to their communities upon graduation. Scholarship recipients signed an agreement to serve rural and remote areas for 2–4 years. |
| Philippines | ||||
| Cristobal and Worley 201250 | Medical graduates from Ateneo de Zamboanga University School of Medicine, Philippines archipelago, Mindanao. More than 160 graduates from 1999 to 2011. |
Students were recruited from the local region of Zamboanga province. Selection methods consisted of a combination of grade point average, Otis Lennon School Mental Ability Test (measures reasoning skills across a variety of skill sets) and an interview. |
Lack of doctors willing to serve in underdeveloped areas. Initiative starting from scratch to provide a solution to address the major health problems of the communities. Apart from remoteness, civil unrest between government forces and rebel groups contributed to the challenges in attracting doctors to work and serve this region. |
Socially accountable medical education to improve the workforce in disadvantaged regions. Graduates of Ateneo de Zamboanga University to address the health needs of the Zamboanga province. Addressed priority health needs such as high birth and infant mortality rates, malnutrition and various infectious diseases. |
| Siega-Sur 201722 |
The population in the Philippines was 102 million, with 44 medical schools in 2016. Most graduates prefer to practice in urban areas, resulting in the maldistribution of doctors. Graduates of the two medical schools in the Philippines: SHS-Palo and a medical school with a more conventional curriculum, were studied for their career choices, practice location, motivation towards community-based service and preparation for addressing their community health priority needs. 13 cohorts from the SHS-Palo between 1989 to 2013 were surveyed. 72 out of a possible 121 graduates participated in the study. |
The SHS-Palo preferentially selects students from the lower socioeconomic class and the rural and remote communities. Students were nominated by their rural communities, which needed health workers. Scholarships are provided to the selected students, and the communities also give some support to their students during their training. Selected students will, in return, serve their communities upon graduation through a social contract arrangement. Selection process emphasised students’ commitment to serve the community more, instead of academic scores and achievement. SHS-Palo waived the normally required National Medical Admission Test as an exemption for students entering its program. Later, as a regulatory requirement, the admission test became compulsory for all students, including the SHS-Palo program, in 2013. Progression is through a competency-based stepladder program. Students enrol and progress from midwifery to nursing, then into medicine. |
SHS-Palo was established with a social accountability mission. It is a founding member of the Training for Health Equity Network partner of medical schools. The university exists for the benefit of the local region, enabling equity in access to health professional education and health services. SHS Palo strives to ensure its graduates address the health needs of the poor and most isolated in a society where doctors and other health workers are scarce. |
Produce socially accountable graduates who have a community-based service attitude and who practice in rural and remote areas. Graduates give back their professional service to the communities that selected and supported them during their training. Graduates to work as rural physicians (district or provincial hospitals or rural government health services) and practice where they will address the priority health concerns of their local community. |
| Labarda et al, 201851 | Graduates of the University of the Philippines Manila-School of Health Sciences. The graduate tracking survey of School of Health Sciences students from 1976 to 2011. More than 2000 health workers were produced during the study period. | The study evaluated the University of the Philippines Manila-School of Health Sciences after 36 years of implementation of its innovative model of selection and training. |
There was no information on factors informing strategy due to the nature of the study. The study reviewed the performance of the University of the Philippines Manila-School of Health Sciences in terms of addressing workforce distribution and inequity. |
Most of the graduates have stayed in their country, and more than half of them have continued to serve in their communities. A significant proportion have remained in primary care facilities. |
| Taiwan | ||||
| Lin et al, 202173 |
513 first-year Taiwanese medical students from seven schools that selected students using both the multiple mini-interview and joint college entrance written test. The seven medical schools participated in this study to compare demographic characteristics and motivations for studying medicine. |
The selection was made based on students’ essential attributes or academic performance. Grade point average in high school, personal essay, English Proficiency Test Score, and performance in the General Scholastic Ability Test were used to choose students for the multiple mini-interview selection pathway. Schools that used the joint college entrance written test pathway ranked students based on their performance scores (grade point average, essay, English Proficiency Test and General Scholastic Ability Test) and subsequently enrolled them primarily based on student ranking. |
Factors informing selection were not explained. The study compared the demographic characteristics and student motivation for studying medicine. |
Consideration for a fit-for-purpose graduate was not stated. None of the selection methods favoured students from diverse backgrounds. |
| Thailand | ||||
| Putthasri et al, 201366 |
19 faculties of medicine graduates in Thailand between 2020 and 2012 convened at the Ministry of Public Health. Three consecutive graduates of the three different admission tracks in Thailand were examined in the study. |
Students in Thailand are selected from the two modes of admission: the normal and special tracks. Under the normal track, any grade-12 student can apply to sit the national entrance examination. Recruitment to study medicine for 6 years was based on competency. There are two components of the special track: %u2022 CPIRD program, targeting students residing in provincial areas %u2022 ODOD program, selecting students from non-provincial cities or rural areas in Thailand. |
The admission pathways are part of the national program to solve the shortage and maldistribution of Thailand’s health workforce. Graduates to fulfil mandatory rural service and obtain higher clinical competency. Heavy penalties apply if the mandatory 3 years of service are not fulfilled: a fine of US$13,000 (~A$18,200) for CPIRD and normal track, and US$65,000 (~A$91,100) for ODOD graduates. |
Mandatory rural service in the severe shortage areas: CPIRD graduates to serve in the provincial areas and ODOD graduates to serve in the rural areas. Graduates of both tracks are allocated to work in their hometowns or their neighboring districts and provinces. Graduates’ rural attitudes are prioritized apart from their medical and public health competencies. |
| Pagaiya et al, 201567 |
Graduates from the years 2000–2007 were studied for 11 years. 7157 doctors graduated and worked with the Ministry of Health between 2000 and 2007. 1093 graduates were from the CPIRD track and 6064 were from the normal track. This study examined the impact of CPIRD on doctor retention in rural areas and public health services. |
Selection methods and approaches as described by Putthasri et al. (2013)66 for Thai medical schools. The CPIRD program targeted students from provincial areas, while the ODOD program selects students from non-provincial cities or rural areas in Thailand. The normal track or conventional approach of selection was based on the National Entrance Examination and student competency assessment. |
The need to retain doctors in provincial and rural areas in Thailand, where the community health needs are high due to a shortage of health workers. | Alternative selection pathways enabled the recruitment of students from the provincial and rural areas and retained them in those rural regions to improve public health services upon graduation. |
| Arora et al, 201768 |
Local medical graduates who started work for the Ministry of Public Health Thailand between 2001 and 2015 were studied. Graduates were trained through a partnership between 14 universities and 37 accredited hospitals under the Ministry of Public Health. 19,338 graduates were employed with the Ministry of Public Health from 2001 to 2015. 5909 (30.6%) of the graduates were from the CPIRD and ODOD programs, and the rest were from the normal track. Factors associated with 3-year retention in the Ministry of Public Health health services were identified. |
A 15-year cohort of graduates from the CPIRD, ODOD and normal-track recruitment programs was studied. The normal track and the two special recruitment programs are outlined in the earlier studies (Putthasri et al, 201366 and Pagaiya et al, 201567). |
Similarly to the previous studies in Thailand, the maldistribution and critical shortages of doctors in rural areas informed the selection approaches. The need to retain doctors in underserved areas where health needs are insufficiently addressed. |
The CPIRD and ODOD programs were intended to recruit and retain graduates in their home provinces and rural areas. Addressing the geographical maldistribution of doctors was a priority. |
| Techakehakij and Arora 201769 |
The study examined the retention of graduates from January 2003 to October 2014 and followed up to June 2015 in Thailand. A total of 15,253 physicians (of which 10,487 graduates are from the normal track), 3989 from the regular CPIRD, 510 from ODOD, 63 non-civil servant graduates with medical-related bachelor’s degrees and 204 graduates with medical-related bachelor’s degrees who are civil servants. |
Recruitment schemes are normal track, CPIRD and ODOD as in the already mentioned studies from January 2003 to October 2014 (Putthasri et al, 201366 and Pagaiya et al 201567). In addition, civil servants who already have a bachelor’s degree and work in the Ministry of Public Health and other postgraduates with medical-related bachelor’s degrees who were not civil servants were recruited. |
Similarly to the other studies in Thailand, the recruitment and retention of doctors in the country’s provincial regions and rural areas were the reasons for the different recruitment programs. |
Retention of physicians within the Ministry of Public Health hospitals and working as rural physicians to serve and address the health needs of rural communities. Increasing retention and lowering resignation rates during the compulsory period of the contractual agreement was desired by the government. |
CPIRD, Collaborative Project to Increase Production of Rural Doctors. ODOD, One District One Doctor. RTME, rural-oriented tuition-waived medical education. SHS-Palo, the University of Manila-School of Health Sciences. SJT, situation judgement test.
Five major themes emerged from the inductive analysis of the included studies: engagement of key stakeholders in the selection approach (political validity), prioritizing the health needs of the communities that medical schools serve (social accountability), responding to the needs of communities in which schools are located (responding to context), ensuring a sustainable selection approach, and a purposive and mission-driven strategy. Some published studies had more than one highlighted theme, and some themes were common among medical schools.
Political validity
The reviewed studies showed that well-designed selection approaches that consider the interests of employers and other stakeholder groups could produce a medical student body that responds to national health workforce needs. Meaningful collaborations with key stakeholders provided rural and disadvantaged communities an opportunity to study medicine in Nepal, the Philippines and Thailand22,24,66,68,69. The formation in Indonesia of the Medical Education Law Number 20 of 2013 guided the selection approach of medical institutions in Indonesia74. The law enabled the incorporation of non-academic attributes in selecting medical students. It allowed institutions to design selection methods to widen participation and meet their country’s workforce requirements74. Policymakers’ engagement shifted selection practices, enabling institutions to meet the government's intention and national needs.
The University of Manila-School of Health Sciences in the Philippines (SHS-Palo) implemented an innovative selection strategy in collaboration with the health sector and the local community22. The country’s needs informed the selection approach, which aligned with the nation’s requirements and the school's mission (Table 4). The approach highlighted the extensive stakeholder engagement in the selection process to address the health needs of the disadvantaged communities.
Thailand strategically aligned three different selection programs to meet the country’s provincial, rural and remote medical workforce needs66,68,69. Table 4 outlines how the Ministry of Education recruits medical students to study in universities. Thailand’s Collaborative Program to Increase Production of Rural Doctors was developed to address shortages in the provincial setting. The One District One Doctor program was initiated to improve services in rural and remote areas. Collaboration between medical schools and government ministries enabled the schools to address the needs of the different geographical regions. The government provided recruitment options for medical students, demonstrating its interest in the wellbeing of the rural and remote communities67.
Co-designed selection schemes can serve national interests but are not without negative effects. The introduction of the Education Plan for Excellent Doctors in China in 2012 underscored the unintended effects of China’s policy changes75. In China’s aspiration to improve the quality of doctors, the ‘quality’ concept led to selection based on high academic achievements. Consequently, more students were selected from urban and higher socioeconomic backgrounds. The policy change reduced student diversity and was counterproductive in addressing the health needs of China’s rural population75.
Social accountability and selection
Published studies featured community engagement in some medical schools (Table 3). Positive motivation towards addressing local priority health issues within their practice location was reported from the graduates of SHS-Palo in the Philippines22. The school preferentially selects students from rural and remote communities and equips them through their stepladder curriculum. The curriculum trains a broad range of health workers, from community health workers to doctors, in a single and sequential continuous curriculum. It allowed students to progress from midwifery into nursing before doing medicine22.
Labarda and Labarda (2018) examined human resources in the Philippines and reviewed how SHS-Palo addressed inequity. Insights from SHS-Palo revealed good progress in graduate retention in primary care facilities. After 36 years of its socially accountable initiative, 90% of SHS-Palo graduates remained in the country, and a significant number continued to serve in their local communities or in primary care level facilities51.
Driven by a socially accountable training mission, SHS-Palo’s stepladder selection program emphasizes students’ commitment to serving their community. Likewise, Nepal’s Patan Academy of Health Sciences medical school implemented multiple selection approaches (Table 4) to achieve an equitable and diverse student body to address the health needs of its disadvantaged communities24.
Responsiveness to context
The reviewed studies illustrated unique contextual responses among LMICs in the Asia-Pacific region. Geographical distribution had a significant impact on some of the approaches. Observed fit-for-purpose selection practices were context-specific in responding to local workforce needs. The Patan Academy of Health Sciences in Nepal, like other medical schools, aligned its student selection to widen representation from disadvantaged backgrounds.
The institution also assessed non-cognitive attributes, student personality and attitudinal traits in its stepwise selection approach (Table 3). Nepal demonstrated that a single selection approach may not adequately meet the aspirations of medical schools, the health sector and the community. The Patan Academy of Health Sciences designed a staged selection approach with a matrix weighted for disadvantaged communities24. The approach was intended to enhance access to medical education, improve the livelihoods of disadvantaged communities and address priority areas of health services.
Western China’s approach in bundling selection with scholarships in Lanzhou University Medical College and the Gansu University of Chinese Medicine attracted rural medical students from low socioeconomic backgrounds71. This initiative followed the 2010 Chinese government reform that supported student tuition and helped with employment upon study completion. Aligning selection with scholarship awards and other incentive schemes attracted doctors to work in areas of critical need71.
Selecting students from the remote regions where medical schools are located has retained rural students within those communities64. Building the Pattimura University Medical School within a rural province shifted selection to ‘favor’ those from the hard-to-reach rural and remote regions in the province of Maluku, Indonesia72. The strategic infrastructure development was a response to Indonesia’s specific context. Locating a medical school in Maluku province drove selection to focus on recruiting students from this vicinity to study in the local medical school (Table 3).
Sustainable selection approach
Some studies revealed the pathways from selection, employment and retention post-graduation. Regardless of the selection approach, the sustainability of the intended outcomes was an important consideration. Studies from Indonesia, Nepal, the Philippines and Thailand demonstrated the role of partnerships and collaborations between government ministries, the health sector, medical schools, communities and local governments to facilitate employment where graduates are most needed22,24,51,66,68,72.
Engaging stakeholders in the selection process resulted in better support for students and graduates in China. Financial support and other benefits rendered to students in rural townships in western China, affirmed the interconnection of selection with the government’s selective admission policy. As highlighted in Table 4, the Ministry of Education in China guided schools on which geographical areas to select students. Implementation of policies for doctors to practice at their place of origin, aligned with the country's rural-to-urban migration restriction, to sustain the workforce64,70.
A mandatory period of compulsory service, to address workforce shortages in rural and remote areas, could serve as a workforce retention measure24. Graduates who gave back their professional service to the communities that recommended and supported them during their training constituted a sustainable selection model in the Philippines22,76. Managing selection as a continuum of the health service could sustain good selection strategies.
Thailand’s ‘beyond selection’ approach ensured that its various recruitment tracks (Collaborative Program to Increase Production of Rural Doctors, the One District One Doctor program and normal recruitment tracks) attracted students committed to working and remaining in the provinces to which they were initially assigned. This strategy reflected the country’s concern with sustaining its workforce by selecting specific groups of students not merely for medical school admission, but with a focus on meeting national healthcare needs (Table 3)68. The country ensured that its selection strategy would impact the health needs of its communities in the immediate future. Such practices, although imperfect, enabled selection policies to facilitate a return on investment in medical training within LMIC settings68. The approach ensured that graduates work in the communities that needed them most after graduation. In Indonesia, rural and remote graduates have a high likelihood of practicing and remaining within the Maluku province72. Even though rural and remote recruitment approaches worked, offering permanent contracts, incentivizing private practice entitlement and other graduate retention measures sustained the intentions of selection strategies72.
Purposive and mission-driven selection
Some studies foregrounded selection to be purposive and mission-driven. The Ateneo de Zamboanga University had a mission to address the health problems of more than three million people in the rural communities in the Mindanao province of the Philippines (Table 4). Its mission-driven model of education contributed to a reduction in the Zamboanga region’s infant mortality rate by about 90% in the 14 years of its existence50. The achievement demonstrated a socially accountable, driven mission.
SHS-Palo’s purposive selection approach was a response to the health problems within the poor and most isolated communities within the Eastern Visayas region of the Philippines (Table 4). The university’s purposive mission guided the preferential selection from the low socioeconomic strata, and rural and remote communities in the region22. Similarly, Upadhyay et al (2017) reported an innovative and purposive selection process at the Patan Academy of Health Sciences in Nepal (Table 3). The academy’s tiered selection approach aligned with scholarship awards for the underprivileged students. It used an inclusive and equitable system to cater to its country’s needs24.
Evidence from Taiwan (Table 3) illustrates how selection methods in seven Taiwanese medical schools did not differentiate students selected through multiple mini-interviews and joint college entrance written tests73. The study revealed that if the intention is to recruit from a wider student background to fulfil the institutional purpose, flexible systems of selection need to be planned before implementation.
Discussion
This scoping review found that, despite the large and growing population in the Asia-Pacific region, relatively few studies focused on medical student selection and a fit-for-purpose workforce. The published evidence was from China, Indonesia, the Philippines, Taiwan, Thailand and Nepal. The lack of studies from the Asia-Pacific region was highlighted in the Ottawa consensus statement on selection and recruitment to the health professions3. Similarly, an absence of evidence from the Pacific was reported in a study that looked at factors associated with increasing rural doctor supply in the Asia-Pacific LMICs49.
Despite these identified gaps, medical student selection practices have provided key insights for medical schools within this populous and diverse region. A proposed selection framework that could potentially be adopted by medical schools across the Asia-Pacific region and similar contexts was developed from the synthesised themes.
Proposed selection framework
The proposed framework is illustrated in Figure 2. It features the five main themes: the mission and purpose of medical schools, social accountability, context, political validity and sustainable selection. The framework closely aligns with the Analysis, Design, Development, Implementation, and Evaluation (ADDIE) model introduced by Cleland et al (2023)77.
There are similarities and key differences between the ADDIE model and this proposed framework. The analysis section of the ADDIE model covers the goal, desired outcome and selection process. The desired outcome refers to an applicant’s relevant knowledge, skills and attitudes. It pointed out the importance of constructive alignment between outcomes and selection. Similarly, the ADDIE model emphasized the mission of medical schools, context and government drivers (political validity) in selecting students77. The same is articulated in this framework to some extent. Moreover, this proposed framework views the selection process more broadly without delving into the details of selection designs and the tools to be used, although these are important in achieving the ultimate selection goals. Both models stressed the significance of monitoring and evaluation of the approach taken.
However, this framework adds the sustainability dimension to reduce the wastage of resources and efforts invested by medical schools and stakeholders towards selection. Additionally, a socially accountable approach is linked to this newly proposed framework. Relevant policies and the desired selection outcomes precede an aligned intentional curriculum. The framework is designed to contribute to producing graduates who can work and thrive in the health systems in the region.
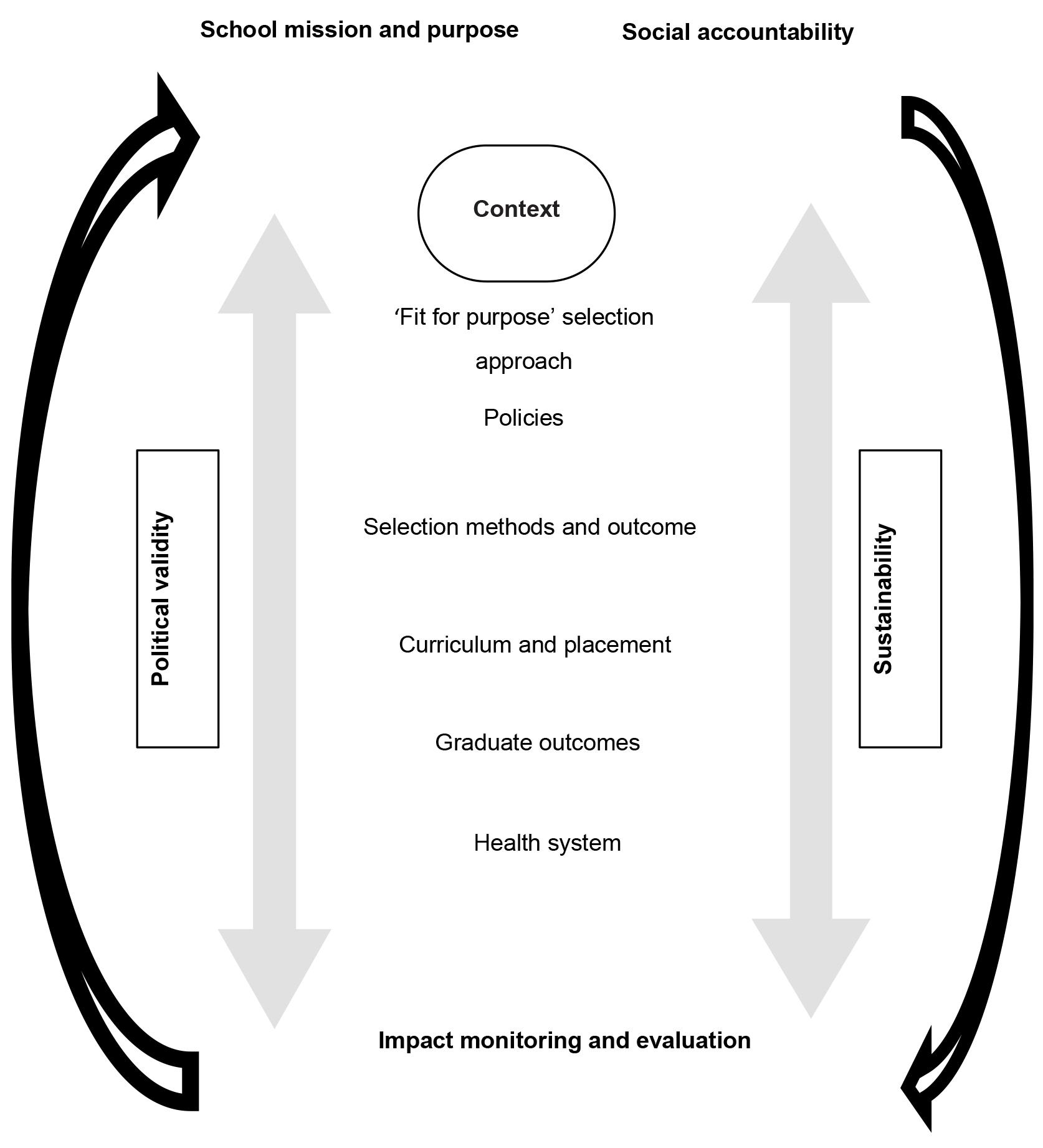 Figure 2: Potential selection framework for medical schools across the Asia-Pacific region.
Figure 2: Potential selection framework for medical schools across the Asia-Pacific region.
School mission and purpose
Experiences in LMICs in the Asia-Pacific region suggest that medical schools define and articulate their school mission better. Socially accountable medical schools had clear missions that translated into their selection approach, curriculum delivery and clinical placements22,50. A study in the US claimed that 40% of medical schools had no mention of diversity-related language in their purpose statement78.
School mission normally dictates selection approaches, which subsequently align with the design of the selection methods. Despite the linkage between social mission and school admissions, Ellaway et al noted that the disconnect remains79. ‘If the commitment to a mission is real and purposive, then its translation to admissions and the ability of admissions to respond needs to be more than an aspiration’ (p. 225)79. Medical schools in the Asia-Pacific region with a clear mission have made some impact on the health services within their communities22,24,50.
Social accountability
WHO defines social accountability of medical schools as ‘the obligation to direct their education, research, and service activities towards addressing the priority health concerns of the community, region, or nation they have a mandate to serve. The priority health concerns are to be identified jointly by governments, health care organizations, health professionals, and the public’(p. 3)79. Some excellent progress in social accountability practices was reported in this review22,24. The Philippines and Nepal are two such examples22,24,51,65,76.
Although medical schools in China, Indonesia and Thailand do not portray themselves to be socially accountable, their student selection practices reflect an intention to address the needs of the rural population66,69,71,72. Despite the positive outcomes reported by medical schools in LMICs, opportunities to integrate social accountability into medical education remain80. Although the social accountability framework has made an impact in the Philippines and other countries, there are opportunities for innovative selection among socially accountable health professional education institutions in the region50,81.
Social accountability and school mission may operate differently. The difference is more obvious in institutions without a social accountability mandate. However, in some schools, mission and purpose drive the institution to be socially accountable39. Social accountability is not an isolated concept; rather, it is intricately connected to the mission and goals of medical schools. Where this has been the case, the community benefits from improved delivery of health services22,50,82,83.
Context
Context is central to guiding institutional mission, purpose, social accountability initiatives and the approach to medical student selection4. The experiences from LMICs in the Asia-Pacific underscored purposive selection designs tailor-made to country priorities and needs22,24,66. Medical schools need to consider the varying contextual factors when implementing the proposed framework in Figure 2.
Population geographical distribution, rural health needs, emigration, training institution locations and government priorities are some factors that influence selection24,64,66,67. In a report from seven Asian countries, tension remained between the use of cognitive and non-cognitive attributes for selection, and balancing this with the school mission and human resource needs84. Despite the differences in contexts and selection approaches, increasing the number of graduates to serve in underserved regions is a shared outcome across most Asia-Pacific LMICs69,71,72,76,85.
Curriculum and placement
Mission and purposes are fulfilled when curricula are specifically designed to meet the intentions of the selection77. Socially accountable medical schools from both LMICs and high-income countries have reported models of community-engaged curricula and their benefits to rural and disadvantaged communities76,86. The curriculum of the Ateneo de Zamboanga University School of Medicine in the Philippines, delivered through community-engaged education, produced graduates who demonstrated commitments to serving in medically underserved areas85.
The goal of the selection process is to produce graduates who meet the health system's needs11,82. Longer community-based rural curricula are ideal instead of the predominant hospital-based curricula design83,86. Thailand’s Collaborative Project to Increase Production of Rural Doctors rural training program attracted and retained doctors in community hospitals where learning had occurred64. A tailored selection approach, when combined with a selection-ready curriculum, could accomplish synergistic outcomes.
Health system and impact monitoring
Framing selection with the graduate outcome in mind draws upon a health system thinking approach and circumvents the temptation to treat selection as a standalone school activity. Previous calls have been made to strengthen health systems by transforming medical education to try to reduce the mismatch between training and community service87. Apart from selecting and equipping graduates with the right skills and competencies, other factors play a role in improving the health system. While the improvements cannot be solely attributed to the services provided by graduates, medical schools can monitor progress or otherwise within their health systems50.
Regular monitoring and evaluation of the selection components outlined in Figure 2 facilitate timely adjustments. Thailand’s review of its Collaborative Project to Increase Production of Rural Doctors and One District One Doctor program led to the ‘inclusive’ track program88. The ‘inclusive’ track addressed the weaknesses encountered with the former approaches. The evaluation of Manila School of Health Sciences' 36-year innovative model of selection (Table 3) revealed that a sizeable proportion of those from poor communities who were meant to benefit from the program did not receive the intended benefit (leakage rate). Some students from high-income families who benefited were not targeted to benefit (under-coverage rates), highlighting the need for monitoring and early intervention51. The evaluation revealed that a significant proportion of students from high income families actally benefited more from the innovative model of selection compared to those from poor families.
Political validity and sustainability
Political validity relates to the engagement of stakeholders in selection system design and development89. It is defined as ‘a measure of the extent to which stakeholders (employers, community, government, and others) consider the selection tools used to be appropriate for use in selection’ (p. 11)90. Some selection practices from the Asia-Pacific region demonstrated multi-sectoral stakeholder-engaged planning to achieve desired goals66,68.
Alignment of selection measures to bonded diversity scholarships and workforce incentive schemes assisted in the retention of doctors where they were needed most66,68,69. Coercive measures were tried in Nepal, Thailand and the Philippines to retain graduates in rural and remote areas22,24,66,74. Stakeholder-supported selection approaches benefited communities in Bangladesh, where incentives were tailor-made for doctors who worked in specific hard-to-reach rural districts91.
Political validity is essential for the proposed framework in Figure 2 to succeed. Politically valid selection policies could minimize negative perceptions and criticisms77. In the Pacific, stakeholder engagement and policy changes are challenging. Although support for selection changes was expressed by staff and key stakeholders in Fiji more than a decade ago, implementation has been slow92. The selection of future doctors is competitive, resource-intensive, and bound to be criticized by students and stakeholders93.
Alignment with stakeholders’ preferences and managing external interference is a challenge for some medical schools in the Asia-Pacific region64,75,91. While government support is essential in the election process, potential negative consequences are to be anticipated by both the institution and the health system51,75,91. For example, the good intentions of producing quality doctors in China through the Education Plan for Excellent Doctors policy resulted in a reduction in its student diversity75. Policy changes have unintended consequences on workforce diversity. This resulted from an aspiration to have a quality workforce without fully defining the quality for their context.
Implications of findings
The majority of the studies were cross-sectional, with variable quality. Opportunities remain for well-designed longitudinal research to determine the role of selection in achieving a fit-for-purpose workforce and its impact on the health outcomes of communities in LMICs. The findings from this scoping review demonstrate the need for medical schools in the Asia-Pacific region to prioritize the connection between the recruitment of medical students and their foreseeable nature of practice and practice locations. This review offers an opportunity to further examine the unique factors across different settings that shape how selection approaches impact the health needs of communitiess.
Empirical studies broadly define a fit-for-purpose medical workforce in terms of the need for doctors’ services in priority geographical locations. The required functions of early-career doctors are equally important and need to be better defined to appropriately address priority health agendas. Supporting junior doctors could assist in meeting the health needs of their disadvantaged communities.
The proposed framework in Figure 2 could assist medical schools in addressing some of the key issues related to selection in the region. A socially accountable approach that is driven by a clear mission and purpose contributes to achieving a fit-for-purpose selection strategy. The context in which selection occurs varies across different jurisdictions. Context-specific factors and the influence those factors have on selection outcomes must be considered. Politically valid selection approaches, when integrated with an appropriate curriculum and student placement system, are feasible in producing desired graduate outcomes.
Stakeholder support enhances the implementation of evidence-based student selection practices. Good selection outcomes could be sustained if retention measures are pre-planned with stakeholders to enable skilled graduates to remain in communities where they are needed most. Alignment of medical student selection policies and methods may subsequently lead to graduate outcomes that are needed by the health system.
Strengths and limitations
This scoping review specifically investigated selection practices within LMICs in the Asia-Pacific region. Studies on this subject are scarce in this region. Contextual relevance is a key strength of this review. The findings could potentially apply to similar LMICs outside the Asia-Pacific region. The pilot searches and consensus of the authors in the inclusion of selected studies to suit the objectives added strength to the review. This review excludes secondary articles, opinions, editorials and commentaries. This may be a potential limitation; however, the scarcity of primary research makes this unlikely. In addition, forwards and backwards reference searches navigated these limitations. The restriction to include documents published only in English is an added limitation of this review.
More than 60% of the studies were cross-sectional, and a similar proportion were of average quality rating (Table 3). Weaknesses were identified in 6 of the 16 criteria laid out in the QATSDD. Two-thirds of the studies didn’t mention an explicit theoretical framework. The stated reliability and validity of the measurement tools and quality of evidence as a result of the measures used were not explained in half of the studies. Twelve studies did not state the research question, although the aims and objectives were mentioned. In explaining the strengths and weaknesses of the studies, comments related to the design and procedures for data collection were generally incomplete. Since the context is specific to the Asia-Pacific LMICs, it may not apply to high-income countries or regions where sufficient doctors are produced to meet the country’s needs. Although the context in the Asia-Pacific may be similar to other regions, geographical proximities were more likely to have influenced practice in each neighboring country from within LMICs and proximal high-income nations.
Conclusion
This scoping review highlights the different selection approaches that medical schools use within the LMICs in the Asia-Pacific region. The lessons learnt from innovative approaches in this region are worth replicating where appropriate.
The engagement of stakeholders in the selection process, premised on a clear mission and purpose, is imperative within each context. A proposed selection framework aimed at contributing to a fit-for-purpose workforce could guide selection approaches in LMICs in the Asia-Pacific region and similar contexts.
Data availability
The data supporting the findings of this study are available on request.
Acknowledgements
The authors extend their gratitude to Mr Stephen Anderson for his support in guiding the search strategy for this scoping review.
Funding
No specific funding was received for this scoping review.
Conflicts of interest
The authors declare no conflicts of interest.
AI disclosure statement
Some portions of the manuscript were supported by an AI-assisted tool. Microsoft Co-pilot 365 v2025 was used to assist with grammar checking and to improve readability of the initial version of the drafted manuscript. Language edits were explored with the tool to improve clarity. All subsequent drafts up to the final version, substantive content, analysis and interpretation are the authors’ own.