


Introduction
Rural healthcare transformation is one of the most pressing challenges in contemporary global health policy. Over 3.4 billion people worldwide live in rural areas, representing approximately 43% of the global population, with the largest concentrations in Asia and Africa1,2. These communities face disproportionate health disparities, characterized by higher mortality rates, an increased burden of chronic diseases, and significantly limited access to quality healthcare services3,4. The intersection of geographical isolation, inadequate health infrastructure, and a shortage of qualified healthcare professionals creates a perfect storm of healthcare inequity in rural settings5. Rural residents experience substantially higher age-adjusted mortality rates for cardiovascular disease, diabetes, cancer, unintentional injuries, and stroke than their urban counterparts6-9. Furthermore, rural populations demonstrate shorter life expectancy and reduced access to preventive healthcare services, compounded by socioeconomic barriers and transportation challenges10,11.
Traditional healthcare delivery models have proven inadequate in addressing these multifaceted challenges, necessitating innovative approaches that leverage technological advancements. The emergence of telehealth and artificial intelligence (AI) presents unprecedented opportunities to revolutionize healthcare delivery in underserved rural communities12,13. Telehealth technologies can dramatically increase patient engagement while reducing travel costs and improving care quality for geographically dispersed populations14,15. Simultaneously, AI applications offer powerful tools for enhancing diagnostic accuracy, enabling remote monitoring, and facilitating personalized treatment plans tailored to rural healthcare contexts16,17. However, the integration of these technologies introduces complex legal, ethical, and regulatory considerations that must be carefully addressed. Issues surrounding patient consent, data privacy, cross-jurisdictional licensing, and algorithmic bias present significant challenges that require comprehensive legal frameworks18,19. The digital divide further complicates implementation, as inadequate internet infrastructure and limited digital literacy may paradoxically exacerbate existing health inequities20,21.
Despite extensive research on the individual components of rural healthcare challenges, there is limited comprehensive analysis examining the intersection of telehealth, AI, and legal frameworks specifically addressing global health equity. This review provides novel insights by synthesizing multidisciplinary perspectives on technology integration, regulatory requirements, and implementation strategies across diverse global contexts. The primary aim of this study was to evaluate how the integration of telehealth and AI can advance global health equity through appropriate legal and policy frameworks. The specific objectives are as follows: examine the current applications of telehealth and AI in rural healthcare settings; analyze the existing legal and regulatory frameworks governing digital health technologies; identify implementation challenges and best practices from global case studies; propose comprehensive strategies for sustainable technology integration that promotes health equity; and recommend policy directions for supporting equitable digital health transformation in rural communities.
Methods
Study design
This narrative review employed a comprehensive approach to examine the integration of telehealth and AI in rural healthcare settings, with a particular focus on legal frameworks and global health equity implications. A narrative review methodology was selected to provide a broad, interpretative synthesis of the existing literature while accommodating the multidisciplinary nature of the topic spanning healthcare, technology, law, and policy domains.
Research question and review scope
This review specifically examined the integration of telehealth and AI within rural healthcare settings, with an explicit focus on the legal and regulatory frameworks that govern their implementation and influence health equity. The guiding research question was, How do existing legal and regulatory frameworks enable, restrict, or shape the integrated use of telehealth and AI in rural healthcare delivery, and what are the implications for equitable access to care?
Search strategy
A comprehensive search was conducted across multiple electronic databases, including PubMed, Web of Science, Scopus, CINAHL, and relevant legal databases. The search strategy employed both Medical Subject Headings (MeSH) terms and free-text keywords, including combinations of "telehealth', "telemedicine', "health equity', "artificial intelligence', "rural healthcare', "health equity', "rural health services', "legal frameworks', "digital health', "policy', "governance', "remote monitoring', "healthcare disparities", and "law or regulatory". The search was limited to English-language publications from 2015 onwards to capture contemporary developments in digital health technology.
Study selection and data extraction
The inclusion criteria encompassed peer-reviewed articles, policy documents, and grey literature addressing telehealth and AI applications in rural settings. Studies were included if they addressed the legal, regulatory, or implementation aspects of digital health technologies in underserved populations. Two independent reviewers (MFHL and OJO) screened the titles and abstracts, and a full-text review was conducted for potentially relevant studies. Data extraction focused on key themes, including technology applications, regulatory frameworks, implementation challenges, outcomes, and policy recommendations.
Analysis framework
Data were synthesized using a thematic framework analysis, combining deductive coding based on the review objectives, with inductive coding derived from recurring patterns in the literature. This approach enabled integration of interdisciplinary evidence on technology, law, and health equity in rural health care. A legal–policy analytical framework guided the synthesis, categorizing studies into four domains: regulatory authorization and professional licensure for AI-enabled telehealth; data governance, privacy, and cross-border data flows; accountability, liability, and ethical oversight in AI-assisted remote care; and equity-oriented legal mechanisms influencing rural healthcare access. This framework supported systematic comparison of how legal structures shape the integration of telehealth and AI, and their implications for rural health equity.
Global rural healthcare disparities
Health and healthcare inequalities denote variations in health and health care among different groups that arise from wider social and economic disparities. Health disparities encompass variations in health outcomes, including life expectancy, mortality rates, overall health status, and the occurrence of health conditions. Disparities in global rural health care synthesize the foundational themes emerging from the thematic analysis that describes the structural determinants of rural healthcare disparities. According to the reviewed literature, demographic vulnerability, geographic isolation, infrastructure deficits, and workforce shortages consistently emerged as high-weight, cross-cutting themes, appearing in most included studies irrespective of country income level. These themes function as context-setting determinants, explaining why rural health systems experience persistent inequities and why conventional service delivery models often fail in non-urban settings. By foregrounding these structural barriers, this study establishes the baseline conditions that shape the feasibility, adoption, and impact of digital and AI-enabled interventions discussed in subsequent sections22,23.
Demographic and geographic context
Rural populations worldwide face unique healthcare challenges that are rooted in their geographic isolation and demographic characteristics. Most rural populations inhabit Asia and Africa, with India and China possessing the largest rural populations worldwide24-26. These communities typically demonstrate lower income levels, higher unemployment rates, and reduced educational attainment than urban populations27,28. These socioeconomic factors directly contribute to poorer health outcomes and reduced healthcare utilization patterns. Geographic dispersion creates fundamental barriers to healthcare access, with many rural residents living at substantial distances from healthcare facilities. Transportation infrastructure is often inadequate, forcing difficult prioritization decisions regarding health needs29,30. Studies have consistently demonstrated that transportation represents a key obstacle to accessing essential services, including maternal and child health care31,32.
Healthcare infrastructure and workforce challenges
Rural healthcare systems worldwide suffer from chronic underfunding and inadequate infrastructural development. Many rural areas lack essential healthcare facilities, including hospitals, diagnostic centers, and specialist services33. This infrastructure deficit is compounded by severe healthcare workforce shortages, with rural communities demonstrating inadequate numbers of primary care providers and specialists34,35. Healthcare professional recruitment and retention in rural areas remain problematic due to professional isolation, limited career advancement opportunities, and inadequate compensation structures36,37. These workforce challenges directly correlate with poorer health outcomes and higher mortality rates in rural communities than in urban areas38,39. As shown in Table 1, various contextual factors significantly impact rural healthcare delivery across different domains.
Legal and regulatory frameworks in rural disparities
By foregrounding these structural and systemic barriers, this section establishes the contextual conditions within which legal and regulatory frameworks operate. Demographic vulnerability, geographic isolation, infrastructure deficits, and workforce shortages are not merely service delivery challenges; they directly shape regulatory feasibility, licensure requirements, data governance needs, and equity-oriented policy design. Understanding these baseline disparities is therefore essential for evaluating how legal frameworks enable or constrain the deployment of telehealth and AI-based interventions in rural settings, which are examined in subsequent sections38,39.
Table 1: Contextual factors to rural healthcare delivery, by domain
| Domain | Primary barriers | Impact level | Potential solutions | Studies/reports |
|---|---|---|---|---|
| Infrastructure | Limited healthcare facilities, poor internet connectivity, inadequate transport | High | Investment in broadband, mobile health units, telemedicine centres |
Turner et al40 Nashwan et al41 |
| Workforce | Physician shortages, limited specialists, high turnover | Very high | Incentive programs, telehealth training, rural medical education |
Al Hassani et al42 Michael43 |
| Economic | Low income, lack of insurance, high treatment costs | High | Subsidised care, health insurance expansion, community health programs |
Al-Worafi44 Kerketta and Balasundaram45 |
| Geographic | Long travel distances, transportation barriers, weather constraints | High | Mobile clinics, air medical services, local health outposts |
Atuoye et al29 Douhit et al30 |
| Social | Cultural barriers, health literacy, privacy concerns | Moderate | Community engagement, health education, culturally appropriate care |
Turner et al40 Nakaji et al46 |
| Technological | Digital divide, limited device access, low tech literacy | Moderate | Digital literacy training, device subsidies, simplified interfaces |
Al Hassani et al42 Nataliansyah et al47 |
Telehealth applications in rural health care
The emphasis on telehealth highlights its significance in the literature as a key solution to the access and workforce challenges mentioned previously. In various study designs and geographic locations, telehealth applications showed significant thematic importance, especially concerning address distance, transportation limitations, and shortages of specialists. The identified application domains – remote consultations, remote patient monitoring, mobile health, and maternal and child health – were determined inductively due to their frequency, empirical backing, and significance to high-burden situations in rural environments. Collectively, these themes demonstrate a shift from broad-access facilitation to more specific, population-targeted applications of digital health technologies that have measurable clinical and public health effects48.
Remote consultations and clinical services
Telehealth has emerged as a critical tool for expanding healthcare access in rural communities, particularly in addressing transportation barriers that traditionally limit access to both primary and specialist care. Remote consultation platforms enable real-time communication between patients and healthcare providers, facilitating diagnosis, treatment planning, and follow-up care without requiring physical travel49-51. Evidence demonstrates significant improvements in healthcare accessibility through the implementation of telehealth. A systematic review by Peyroteo et al (2021) indicates that telehealth can substantially extend healthcare access for patients with transportation difficulties, leading to improved clinical outcomes for diverse medical conditions52. Remote consultations are particularly effective for managing chronic diseases, mental health services, and routine primary care needs53-55.
Remote patient monitoring systems
Remote patient monitoring is a transformative approach to chronic disease management in rural settings. These systems enable continuous surveillance of patient health parameters, providing real-time data to healthcare professionals while empowering patients to actively participate in their care management56,57. This technology is especially valuable for managing conditions such as diabetes, hypertension, and heart failure, where consistent monitoring significantly impacts outcomes58. The integration of Internet of Medical Things devices facilitates comprehensive data collection and transmission through connected devices, potentially improving treatment adherence and enabling early intervention in complications59. Such systems ensure continuity of care while reducing the need for frequent healthcare facility visits, addressing both access and cost barriers common in rural settings60.
Mobile health solutions
Maternal and child health has become a specific and prioritized focus area since it is a high-risk field where delays in care are strongly linked to avoidable morbidity and mortality. Research consistently emphasized that digital maternal and child health initiatives are both practical and effective in rural areas, especially for early risk identification, ongoing care, and specialist assistance. In contrast to other telehealth applications, these specific uses were more often associated with tangible outcome enhancements and greater intergenerational health advantages, warranting their targeted analysis within the thematic framework61,62. Mobile health applications leverage smartphone technology to deliver healthcare services directly to rural populations, helping to bridge the digital divide that often exacerbates health disparities63. The mWellcare program exemplifies successful mobile health implementation, demonstrating effective chronic disease management for conditions such as hypertension and diabetes in resource-limited settings57. However, mobile health success depends critically on overcoming implementation barriers, including limited technology access and low health literacy among target populations64,65. Effective programs must address these challenges through comprehensive user education and culturally appropriate interface design66.
Telehealth in maternal and child health
Telehealth applications show promises for improving maternal and child health outcomes in rural communities, where access to obstetric and pediatric specialists is often severely limited. Evidence indicates that telemedicine enables early monitoring and timely interventions, which are essential for reducing maternal and infant mortality rates67,68. Digital maternal early warning systems have demonstrated significant potential for improving maternal health management in rural settings, although challenges persist in translating technological capabilities into measurable health improvements69. Success requires addressing broader socioeconomic factors that contribute to rural health disparities, beyond technological implementation alone70.
Regulatory and legal considerations in telehealth
The effectiveness of telehealth in addressing rural healthcare inequities is strongly conditioned by regulatory and legal frameworks governing professional licensure, reimbursement, data protection, quality of care, and equity. Restrictive licensure laws and fragmented jurisdictional regulations often limit cross-regional telehealth practice, disproportionately affecting rural populations with limited specialist access. Inadequate or inconsistent reimbursement policies further constrain telehealth sustainability by discouraging provider participation. At the same time, telehealth raises critical legal concerns related to patient privacy, data security, and informed consent, particularly in rural settings where digital infrastructure and literacy may be limited. Unclear liability and quality-of-care standards can deter adoption by healthcare professionals, while poorly designed regulations risk reinforcing the digital divide. Consequently, telehealth’s capacity to advance rural health equity depends on coherent, flexible, and equity-oriented legal frameworks that balance innovation with patient safety, data governance, and inclusive access71,72.
Artificial intelligence in rural healthcare innovation
The discussion of AI builds upon earlier themes by examining how advanced data-driven tools may augment limited human and infrastructural resources in rural health systems. While less mature than telehealth, AI-enabled diagnostics, predictive analytics, and administrative optimization emerged as strategically significant themes with growing representation in literature. These applications are framed as mechanisms for compensating for specialist scarcity, improving clinical decision-making, and enhancing system efficiency under resource constraints. The thematic progression from clinical to administrative domains reflects a deductive logic that positions AI as an integrative enabler of broader health system transformation rather than a standalone intervention73-76.
AI-powered diagnostic tools
AI applications in rural health care primarily focus on advanced diagnostic capabilities that can compensate for the limited availability of specialists. AI-powered diagnostic tools, particularly those that utilize image recognition and predictive analytics, demonstrate significant promise for disease detection and risk assessment in resource-constrained environments77,78. Image recognition technologies are especially valuable in radiology and dermatology applications, enabling rural practitioners to achieve specialist-level diagnostic accuracy for conditions such as skin cancer, pneumonia, and other radiologically evident diseases79-81. These capabilities are particularly crucial in rural areas, where access to specialists remains severely limited or non-existent82. Predictive analytics further enhances rural healthcare delivery by analyzing patient data to identify individuals at high risk for chronic diseases, facilitating timely interventions, and improving resource allocation efficiency83. This capability enables healthcare systems to focus limited resources on high-risk populations, potentially improving outcomes while managing costs effectively84.
Precision medicine and drug development
AI technologies accelerate drug discovery and development processes, potentially addressing health challenges specific to rural populations that may be understudied because of limited research funding and resources85. Traditional drug development is lengthy and expensive, but AI can expedite the identification of potential therapeutic candidates through the efficient analysis of large datasets86. Furthermore, AI enables precision medicine approaches that tailor treatments to individual genetic profiles, potentially increasing their therapeutic effectiveness87. This personalized healthcare approach is particularly valuable for addressing the diverse health needs of heterogeneous rural populations88.
AI-driven healthcare administration
Administrative applications of AI are crucial for optimizing resource utilization and operational efficiency in rural healthcare settings, where resources are typically scarce and budgets are constrained. AI-driven systems can analyze patient flow patterns, staffing requirements, and resource utilization to enhance the overall efficiency of healthcare delivery89. AI also contributes significantly to healthcare workforce development by identifying skill gaps and training needs, enabling the design of targeted education programs that ensure rural health workers remain competently equipped to deliver quality care90. E-learning platforms facilitate continuing professional development opportunities, increasing training accessibility for health workers in remote locations91. Table 2 shows various AI applications across different healthcare domains in rural settings.
Legal and regulatory challenges in AI adoption
The adoption of AI in health care presents significant legal and regulatory challenges, particularly in rural settings where institutional capacity and governance structures are often limited. Key concerns include the absence of clear regulatory approval pathways for AI-based clinical tools, uncertainty regarding liability and accountability for AI-assisted decision-making, and insufficient standards for transparency, explainability, and clinical validation92. AI systems rely heavily on large volumes of health data, raising critical issues related to data ownership, consent, privacy, and cybersecurity, especially in contexts with weak data protection enforcement. Algorithmic bias and the limited representation of rural populations in training datasets further risk exacerbating existing health inequities. Additionally, workforce readiness and regulatory recognition of AI-supported clinical roles remain underdeveloped, constraining safe and effective implementation. Addressing these challenges requires adaptive legal frameworks that integrate ethical oversight, equity safeguards, robust data governance, and clear accountability mechanisms to ensure that AI adoption strengthens rather than undermines rural health systems93,94.
Table 2: AI applications in rural health care, by clinical domain
| Clinical domain | AI technology | Primary function | Implementation status | Evidence level | Studies/reports |
|---|---|---|---|---|---|
| Radiology | Image recognition algorithms | Chest X-ray analysis, CT interpretation | Pilot programs | Moderate |
Shinners et al95 Chidi et al96 |
| Dermatology | Computer vision systems | Skin lesion classification, melanoma detection | Research phase | Strong |
Temsah et al97 Jaremko et al98 |
| Cardiology | ECG analysis algorithms | Arrhythmia detection, risk stratification | Limited deployment | Moderate |
Whittlestone et al99 Nittari et al100 |
| Ophthalmology | Retinal imaging AI | Diabetic retinopathy screening | Active implementation | Strong |
Hao et al90 Chidi et al96 |
| Pathology | Digital pathology systems | Histological analysis, cancer diagnosis | Early adoption | Moderate |
Shinners et al95 Jaremko et al98 |
| Emergency medicine | Triage algorithms | Risk assessment, resource allocation | Pilot studies | Limited |
Temsah et al97 Nittari et al100 |
| Mental health | Natural language processing | Depression screening, suicide risk assessment | Development phase | Limited |
Whittlestone et al99 Lehman et al101 |
| Pharmacy | Drug interaction systems | Prescription safety, dosing optimisation | Widespread use | Strong |
Chidi et al96 Gerke et al102 |
Legal and regulatory frameworks
Taken together, the themes outlined across these parts of the review form an explicative narrative that moves from structural inequity, through technological intervention, toward system-level implications. The identification of persistent rural disparities establishes the necessity for alternative models of care delivery, while the analysis of telehealth and AI highlights both their potential and their limitations in the absence of supportive governance frameworks103. These findings directly inform the policy and legal considerations that follow, particularly in relation to infrastructure investment, workforce regulation, reimbursement mechanisms, data governance, and equity-oriented digital health strategies. Grounding policy and legal recommendations in empirically derived themes ensure alignment with the operational realities of rural healthcare systems104,105.
Cross-jurisdictional licensing and practice standards
The regulation of telehealth practice across jurisdictional boundaries represents one of the most significant legal challenges facing rural healthcare delivery systems. Telehealth frequently involves practitioners providing care to patients in jurisdictions other than their primary licensure locations, raising complex questions regarding professional licensing requirements and applicable legal standards83,84. Many countries have begun adapting their legal frameworks to accommodate telehealth practices, with some jurisdictions temporarily relaxing regulations during the COVID-19 pandemic to improve healthcare access106,107. However, regulatory inconsistency creates confusion and may impede comprehensive telehealth implementation, particularly for providers who are uncertain about their legal obligations when treating patients remotely108.
Data privacy and security requirements
The integration of AI into health care raises critical legal considerations regarding data privacy and security, particularly because AI applications typically require extensive collection and analysis of sensitive patient information109,110. Healthcare data handling must comply with stringent data protection laws, such as the General Data Protection Regulation in Europe and the Health Insurance Portability and Accountability Act of 1996 in the US111,112. Legal frameworks must evolve to ensure that AI applications in health care remain transparent and accountable while maintaining patient privacy protection. The potential for AI algorithms to inadvertently encode bias is a particular concern, as such bias could result in discriminatory patient outcomes113,114.
Professional liability and accountability
The integration of AI-driven clinical decision support systems introduces complex questions regarding professional liability and accountability when these systems contribute to diagnostic or treatment errors32,115. Healthcare professionals may struggle to determine liability allocation when AI systems influence clinical decisions, particularly if the algorithmic decision-making process remains unclear116. Clear legal frameworks must address these accountability challenges while ensuring that AI implementation enhances, rather than compromises, patient safety. Guidelines must establish appropriate standards for AI system validation, ongoing monitoring, and professional responsibility in AI-assisted clinical decisions117,118.
Interoperability and data exchange standards
Legal frameworks supporting interoperability are essential for developing integrated health systems capable of effective information sharing across different platforms and providers. This capability remains crucial for care coordination, particularly for patients with complex health needs who interact with multiple healthcare providers119. Standardized data exchange protocols can reduce healthcare access disparities by improving communication and collaboration among providers, ultimately contributing to enhanced health equity120. Legal requirements for interoperability must balance accessibility, privacy protection, and security considerations121.
Implementation strategies and best practices
To effectively address persistent healthcare disparities in rural populations, it is critical to develop and implement targeted strategies that are evidence-based, contextually relevant, and aligned with existing legal and regulatory frameworks. Understanding the barriers to care, including infrastructural, workforce, financial, and policy constraints, allows for implementation practices that enhance the quality and sustainability of healthcare delivery in underserved areas. This section outlines best practices and implementation strategies drawn from recent literature, with attention to regulatory context, to promote successful health interventions in rural settings122-124.
Global case studies and successful models
Successful telehealth and AI implementation in rural settings has been demonstrated across both developed and developing countries. The examples included in Table 3 were selected based on three criteria: documented impact on rural health outcomes, representativeness of regional and system-level diversity, and available information on the interaction between program implementation and local legal or regulatory frameworks.
Table 3: Successful rural digital health implementations, by country
| Country | Program | Technology platform | Target population | Key outcomes | Sustainability factors | Regulatory Context | Studies/reports |
|---|---|---|---|---|---|---|---|
| India | eSanjeevani | Telehealth platform | Rural patients nationwide | 60% reduction in patient travel | Government funding, scalable infrastructure | Supported by national telemedicine guidelines enabling cross-state consultations |
Saberi et al125 World Bank126 |
| Kenya | MobileODT | AI cervical cancer screening | Rural women | 40% increase in screening rates | Partnership with health ministry | Regulatory approvals for AI diagnostic devices facilitated clinical deployment |
Government of India127 Narwadiya and Rao128 |
| Rwanda | Babyl | AI virtual health assistant | General population | Improved primary care access | Health insurance integration | Government digital health strategy provides legal framework for teleconsultations | Peterson et al129 |
| US | Project ECHO | Specialist teleconsultation | Rural providers | Enhanced provider skills | Academic medical centre support | Licensure compacts and reimbursement policies support interstate telehealth | Mink and Peterson130 |
| Brazil | Telessaúde | Telehealth network | Underserved communities | Increased specialist access | Federal health system integration | Federal telehealth regulations shaped network rollout and reimbursement mechanisms |
Percept Actuaries and Consultants131 Taylor132 |
| Australia | Royal Flying Doctor Service | Telemedicine platform | Remote communities | Reduced emergency evacuations | Long-term government commitment | State and federal licensing, scope-of-practice regulations, and telehealth policies guided program development |
University of New Mexico133 Stoumpos134 |
Lessons learned and critical success factors
Implementation experiences across these diverse settings highlight several critical success factors for sustainable rural digital health programs. Beyond context-specific adaptation to local healthcare workflows and cultural factors, alignment with legal and regulatory frameworks is essential to ensure operational feasibility, cross-jurisdictional compliance, and long-term scalability135,136. Infrastructure development and connectivity improvements remain fundamental prerequisites, with evidence showing that intelligent network deployment significantly enhances telehealth effectiveness137. Comprehensive workforce training, digital literacy development, and regulatory compliance education are necessary to enable healthcare professionals to safely and effectively utilize these technologies138. Sustainability and financing mechanisms, including government or public–private partnerships that integrate regulatory requirements, remain critical challenges. Successful programs develop viable long-term financing and policy-aligned models to ensure continued operation, particularly in resource-limited settings where initial implementation often depends on external support139,140.
Challenges and barriers to implementation
The challenges encountered in the implementation of healthcare services in rural areas are intricate and multifactorial, encompassing geographic, financial, workforce, technological, cultural, legal, and regulatory dimensions. These challenges are not treated as isolated obstacles, but as interdependent factors that shape adoption, scalability, and long-term effectiveness. Identifying these constraints provides an essential bridge between empirical evidence and normative analysis, establishing the practical, institutional, and legal considerations that must be addressed through targeted policy interventions and regulatory frameworks in subsequent recommendations141.
Technological and infrastructure barriers
Rural areas frequently suffer from inadequate technological infrastructure, particularly limited internet connectivity and unreliable power supplies, which significantly constrain the potential for telehealth and AI implementation142,143. The digital divide creates fundamental barriers to technology adoption, as communities with poor internet access cannot effectively participate in telehealth programs144. Infrastructure limitations extend beyond connectivity and include inadequate device availability, technical support services, and regulatory guidance (Fig1). Many rural healthcare facilities lack the technological resources necessary to support advanced AI applications and maintain sophisticated telehealth platforms145.
Workforce and training challenges
Healthcare workforce preparation is a significant barrier to technology adoption in rural settings. Many rural healthcare providers have limited exposure to AI and advanced telehealth technologies, potentially impeding the acceptance and integration of these tools into clinical practice146. Effective implementation requires comprehensive training programs that address both technical skills and workflow integration. Healthcare workers need ongoing support and education to effectively utilize new technologies while maintaining quality patient care standards147.
Financial and economic barriers
Cost considerations create substantial barriers to technology implementation in rural healthcare settings, where facilities typically operate under constrained budgets and limited financial resources. The initial capital investment required for telehealth infrastructure and AI systems may be prohibitive for many rural healthcare organizations148,149. Long-term sustainability requires viable financing mechanisms that address implementation costs, ongoing operational expenses, and compliance with relevant policy or regulatory requirements. Many rural areas lack the economic base necessary to support advanced technological infrastructure without external assistance148,150.
Social and cultural barriers
Cultural factors, community acceptance, and governance significantly influence technology adoption in rural areas. Some communities may demonstrate resistance to digital health technologies because of privacy concerns, a preference for in-person care, or limited familiarity with technology151. Effective implementation must address these concerns through community engagement and culturally appropriate program design. Building trust and demonstrating value require ongoing communication and community involvement in program development152,153.
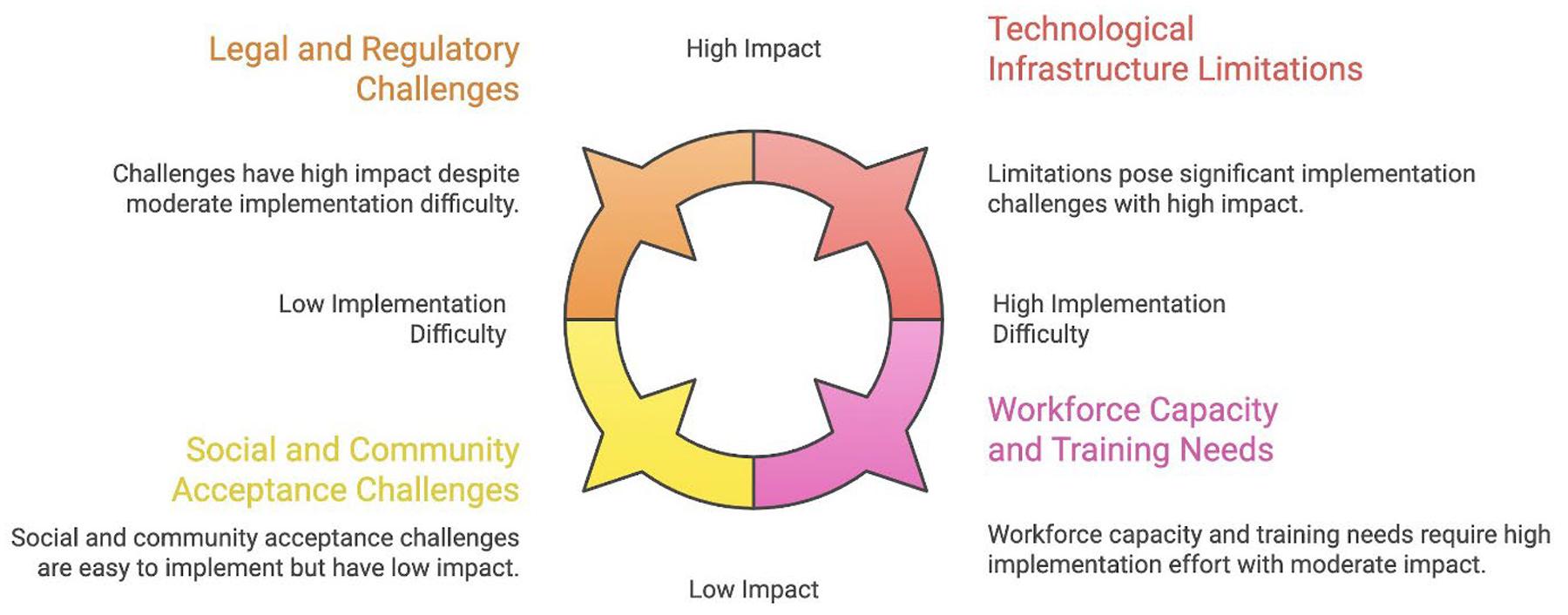 Figure 1: Challenges to technology implementation in rural health care.
Figure 1: Challenges to technology implementation in rural health care.
Policy recommendations and future directions
The ongoing disparities in health outcomes and access to care in rural areas necessitate comprehensive policy strategies to enhance healthcare delivery, specifically focusing on telehealth and AI implementation. Previous analyses have identified numerous barriers affecting rural populations, including geographic isolation, workforce shortages, financial constraints, technological divides, and cultural factors. These complexities demand targeted policy frameworks that prioritize health equity and optimize the adoption and sustainability of telehealth and AI solutions. This section outlines policy recommendations and future directions specifically tailored to support telehealth and AI in rural settings154.
Strengthening legal and regulatory frameworks
Comprehensive policy development must address the complex legal challenges associated with the implementation of telehealth and AI in rural health care. International and regional coordination efforts should focus on standardizing telehealth practice requirements while ensuring compliance with data privacy and ethical standards155. Regulatory frameworks must evolve to accommodate technological advances while maintaining appropriate patient protection standards. This includes developing clear guidelines for AI validation, ongoing monitoring, and professional accountability, ensuring that rural healthcare systems can safely integrate these digital solutions95.
Infrastructure investment and development
Strategic infrastructure investment is a fundamental requirement for successful telehealth and AI deployment in rural settings (Fig2). Government and private sector collaboration must focus on expanding broadband access, enhancing connectivity, and developing reliable telecommunications infrastructure in underserved areas. Investment priorities should target cost-effective, scalable, and sustainable telehealth and AI technologies tailored to resource-limited environments156.
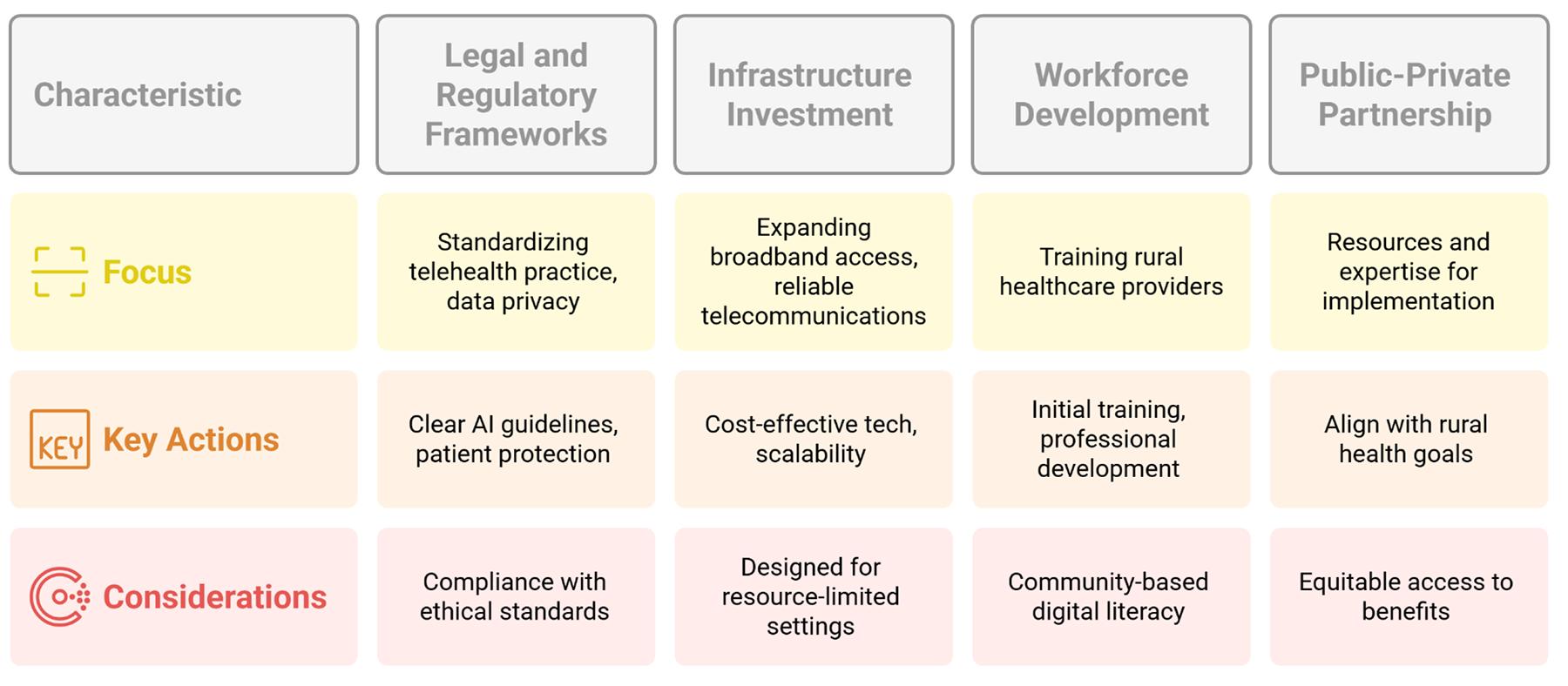 Figure 2: Digital health implementation strategies.
Figure 2: Digital health implementation strategies.
Workforce development and capacity-building
Workforce development programs must address the specific training and support needs of rural healthcare providers implementing telehealth and AI solutions. This includes both initial technology training and ongoing professional development to maintain competency157. Community-based digital literacy initiatives can further support the adoption of telehealth and AI by increasing understanding and acceptance among rural populations158.
Public–private partnership development
Strategic partnerships between public health systems, private technology companies, and international development organizations are essential to provide the necessary resources and expertise for telehealth and AI implementation159-161. These collaborations should align with sustainable rural health goals and ensure equitable access to technological innovations162. Clear governance structures and shared accountability mechanisms are critical to ensure that telehealth and AI solutions effectively address local healthcare needs163-165.
Limitations
This narrative review has several limitations that should be acknowledged when interpreting its findings and recommendations. First, the rapid pace of technological development in telehealth and AI means that some included studies may not reflect the most current technological capabilities or implementation experiences. The field evolves quickly, and evidence from older studies may have limited applicability to current practice. Second, the heterogeneity of rural settings across countries and healthcare systems limits the generalizability of specific implementation strategies. Rural communities in developed countries face different challenges than those in low- and middle-income countries, and successful approaches in one context may not translate directly to others. Third, the narrative review methodology, while providing a comprehensive synthesis across disciplines, lacks a systematic approach and bias assessment of systematic reviews. The selection of the included studies may reflect author bias, and the synthesis may not capture all relevant evidence in the field. Additionally, much of the available evidence comes from pilot programs or short-term implementations, limiting our understanding of long-term sustainability and outcomes. The lack of robust economic evaluations across studies makes it difficult to comprehensively assess cost-effectiveness. Finally, the focus on published literature may introduce publication bias, potentially overemphasize successful implementations while under-reporting challenges or failed programs. Grey literature and unpublished experiences may contain valuable insights that are not captured in this review. Future research should address these limitations through systematic reviews of specific implementation aspects, long-term outcome studies, and comprehensive economic evaluations of rural digital health programs.
Conclusion
The integration of telehealth and AI into rural health care represents a transformative opportunity to address longstanding health disparities and advance global health equity. This review demonstrates that these technologies offer significant potential for improving healthcare access, quality, and outcomes in underserved rural communities worldwide. Telehealth applications, including remote consultations, patient monitoring, and mobile health solutions, have proven effective in overcoming geographical barriers and extending specialist care to rural populations. Similarly, AI-powered diagnostic tools, predictive analytics, and precision medicine approaches enhance clinical decision-making in resource-constrained environments. However, successful implementation requires addressing substantial challenges, including inadequate infrastructure, workforce training needs, regulatory inconsistencies, and financial constraints. Evidence indicates that context-specific adaptation, comprehensive legal frameworks, and sustained investment in infrastructure and capacity-building are essential for sustainable success. Legal and regulatory frameworks must evolve to address cross-jurisdictional licensing, data privacy protection, and professional accountability while ensuring equitable access to technological benefits. Public–private partnerships and international collaborations will be crucial for scaling successful models and sharing best practices across diverse settings. Looking forward, achieving the transformative potential of these technologies requires a collective commitment from policymakers, healthcare providers, technology developers, and communities. Success depends not only on technological innovation but also on comprehensive approaches that address the social determinants of health, cultural factors, and economic barriers.
The vision of equitable healthcare access for all rural populations remains achievable through the thoughtful integration of technological innovation with robust legal frameworks, sustainable financing mechanisms, and community-centered implementation strategies. By prioritizing equity and accessibility in digital health development, we can ensure that technological advances serve to bridge rather than widen healthcare disparities, creating a future where quality health care truly becomes accessible to all, regardless of geographic location.
Funding
This research received no external funding.
Conflicts of interest
The authors declare that they have no conflicts of interest
AI disclosure statement
The authors acknowledge the use of Paperpal (https://paperpal.com), an AI-powered academic tool, for language editing and academic paraphrasing to enhance the clarity and readability of the manuscript. This assistance was limited to linguistic refinement, and the intellectual content, analysis, and interpretations remain entirely the authors' own.
References
You might also be interested in:
2022 - Telehealth use in rural and remote health practitioner education: an integrative review
2018 - Self-efficacy level among patients with type 2 diabetes living in rural areas